SHM Converge 2023
More Data, Fewer Problems
Reducing variability of structured interdisciplinary rounds
Thomas Grogean, Do
✉ tgrogean{@}bhs1.org
William Demarco, DO
✉ wdemarco{@}bhs1.org
Background
Accountable Care Units (ACU® care model) with Structured Interdisciplinary Bedside Rounds (SIBR® rounds), which we consider the gold standard of acute inpatient care, have shown significant improvements in throughput, clinical outcomes, and satisfaction.
Yet, prior studies have noted difficulties achieving similar improvements or sustaining them. Interdisciplinary rounds are a predominantly physician-led teamwork process with efficacy vulnerable to inconsistent physician leadership and engagement. Our hospital had previously implemented ACUs and SIBR, with variable physician and nurse performance and engagement barriers to sustained improvements. SIBR had degraded over the years since launch, predominantly as a result of:
- frontline staff changes,
- organizational leadership changes,
- the impact of a new EMR on work practices
- resource availability to orient and upskill staff
- the impact of COVID-19 on day-to-day care.
In 2022 we began to relaunch our ACUs with SIBR rounds to align unit outcomes with organizational goals: improved length of stay (LOS), discharge coordination, and patient experience. With this relaunch, we sought to optimize process fidelity and outcomes by (1) measuring performance variation and (2) coaching outlier physicians.

What are SIBR Rounds?
- Patient-centered, 6-step communication protocol for hospitalist, nurse, and available allied health to review checklists at the bedside and synthesize plans of care and discharge
- Part of the award-winning Accountable Care Unit (ACU) teamwork care model developed at Emory University in 2010 and now supported by 1Unit Inc.
Methods
We began with the usual project management, online & onsite training, and external expertise to launch on 2 units in summer 2022.
- Oncology unit, 17 beds
- Progressive Care Unit, 20 beds
Then we added a novel strategy:
- Measure: Track daily data on rounds quality and quantity, with the help of the unit’s charge nurse
- Report: Automated hospitalist, team, and unit performance reports, using specialist software
- Act: Physician and nurse leaders review reports weekly to address emerging issues
For 7 months, ~89% of daily team rounds were evaluated across the 2 units (n = 426/477).
Results
Strong results were observed across the triple aim: Patient Experience, Care Outcomes, and Throughput/Costs.
Process monitoring enabled leaders to rapidly remediate performance variability. The SIBR quantity & quality criteria are recorded each day by the charge nurse who is coordinating the SIBR round. The data is digitized by the unit administrator later in the morning, which takes approximately 60 seconds.
Leaders reviewed the reports weekly and intervened as needed – e.g., coaching outlier physicians, upskilling residents or reinforcing education points with nurses – which improved metrics such as duration and quality.
Where necessary, leaders reviewed the full set of data for the day(s) including any custom notes that have been added by the charge nurse to gain a better understanding of the context of the work environment that day and the issues highlighted, see example SIBR notes below.


“SIBR went well today, we had a great first full week. More good catches today from nursing, r/t bowel regimes and anticipated discharge needs for some. Everyone seems very invested in starting on time and what there (sic) role is.”
– SIBR Rounds Manager
“We had a lot of teaching during SIBR today that took up a lot of time. Also, the structure was not followed at the beginning, and I needed to redirect everyone, including nursing to the structure of SIBR. … I will address this asap! ”
– SIBR Rounds Evaluator
“Dr. X was awesome, he called each family while rounding and was still able to finish in 60min. He did a great job!”
– SIBR Rounds Evaluator
Process Metrics – Duration & Quality
Significant variation in round duration was identified between Hospitalists. Hospitalist specific box-and-whisker plots were generated to highlight the intra-group variation.
For example, it was found that some Hospitalists were not adhering to the SIBR ground rule of coming prepared to SIBR. Instead they were completing their primary data gathering at the bedside requiring the rest of the SIBR participants to wait before beginning the 6-step SIBR communication protocol. This was a cause of frustration for the other team members.
With these insights, Leaders are able to intervene and reset the expectations around coming to SIBR fully prepared. Why the focus about ‘Starting on time’? If there are delays in the round beginning, staff become frustrated and will start to question the value of the process when they have other responsibilities.

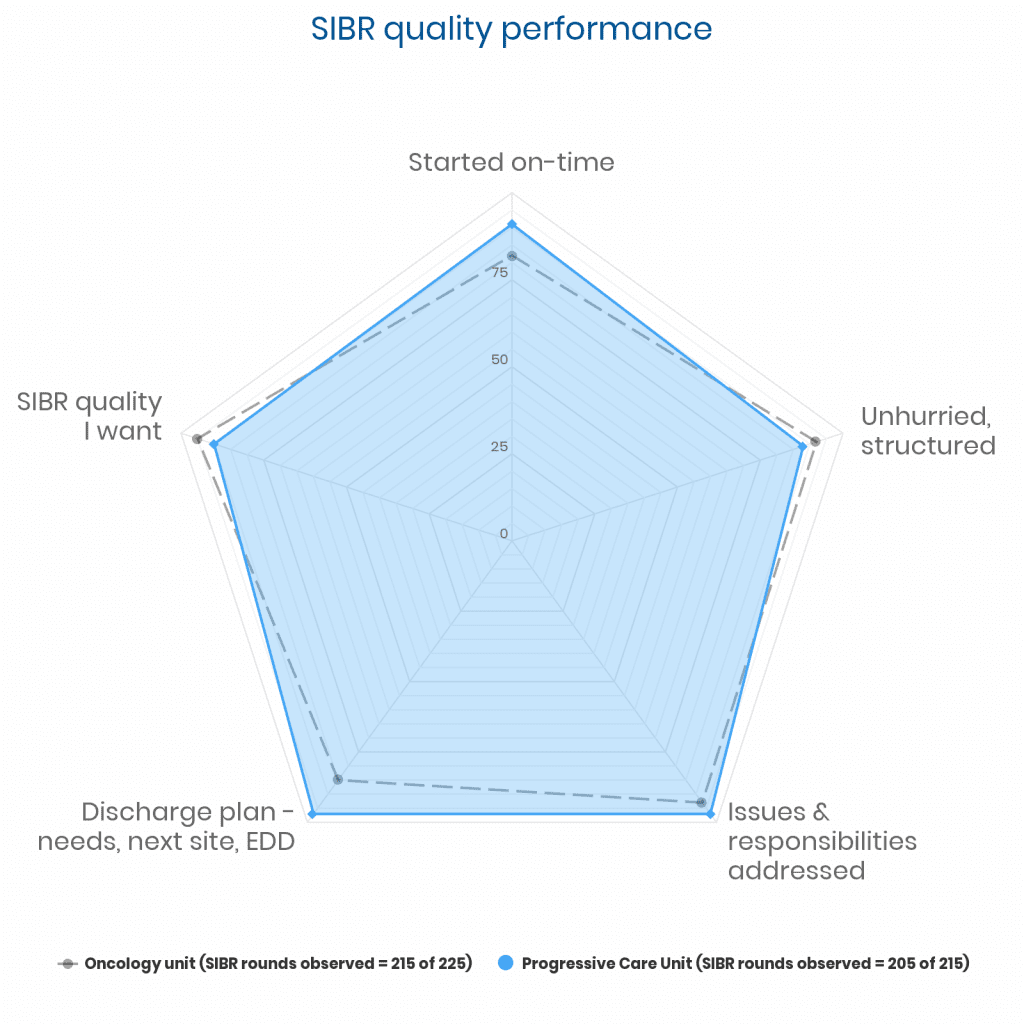
While the overall SIBR quality scores for both units are high, this level of performance is only achieved because of timely interventions when dips in performance are efficiently addressed.
For example, as part of the process monitoring, if it is reported that ‘SIBR did not start on time’ a trigger alert is sent to the SIBR supporting team who can then notify the unit leaders about an issue to address, or to commend the team on continuing to deliver SIBR rounds when faced with challenges.
“SIBR started 1/2 hr late hospitalist assessed pt’s during rounds greater than 5 min a pt. It took 89 min for SIBR on only 8 pt’s – too long.”
– SIBR Rounds Manager
Looking at the SIBR quality data for the ONC unit, the rate of ‘adequately addressing the discharge plan’ criteria in the first month after launch was 73%, two months after launch it was 91% and three months after launch it was 93%, where it has remained at a minimum each month.
Clinical & throughput outcomes
SIBR Rounds with daily quality data showed improvements in unit-level clinical, throughput outcomes on the PCU unit, with significant improvements in patient experience scores on the ONC unit.| ONC | Pre | Post | ±% |
|---|---|---|---|
| LOS | 5.4 | 5.1 | -4% |
| Falls† | 5.3 | 3 | -42% |
† – per 1000 patient days, ^ 3 months pre & 6 months post-SIBR
| PCU | Pre | Post | ±% |
|---|---|---|---|
| LOS | 6.74 | 6.01 | -11% |
| Mortality† | 13.6 | 10.4 | -23.7% |
| 30-day readmits | 17.66 | 16.4 | -7% |
| Falls† | 2.4 | 1.1 | -51% |
| Orders by 9 DC by 11 | 48.8% | 69.4% | +42% |
| Active foley orders† | 416.9 | 395.6 | -5.2% |
† – per 1000 patient days, ^ 3 months pre & 6 months post-SIBR
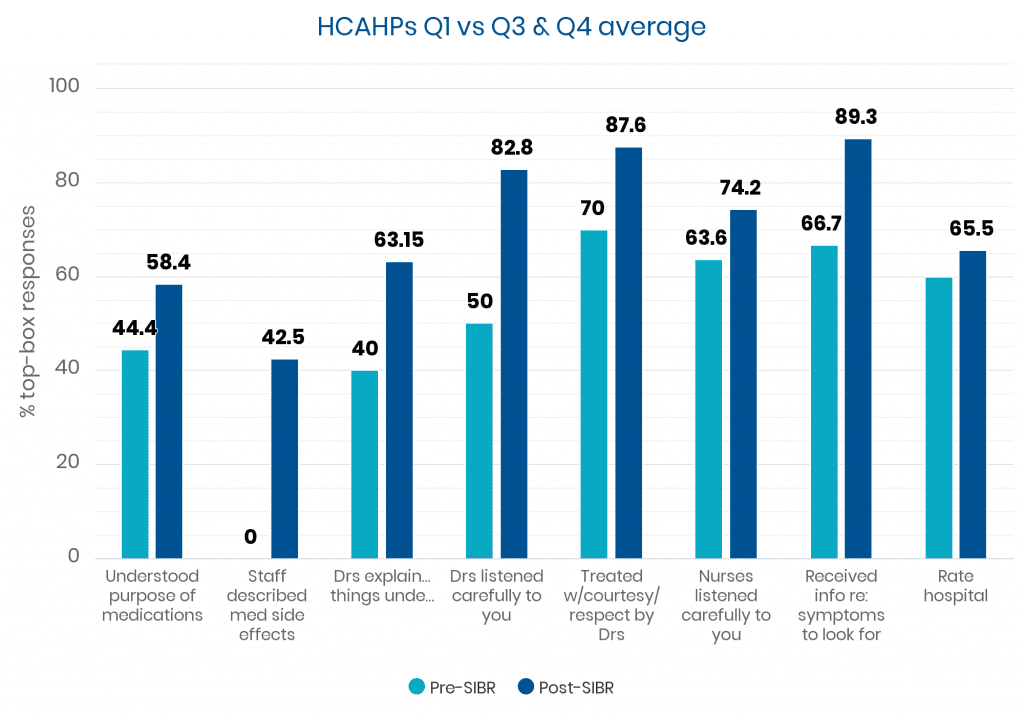
Patient satisfaction outcomes
Unfortunately, the hospital changed HCAHPs systems at the end of 2021 so no older data is available for comparison. Consequently, the HCAHPs ‘pre’ data is limited to the first three months of 2022, with the ‘post’ data being July – December 2022.
The patient population on the PCU limits the numbers that are discharged and suitable for survey attribution to the PCU. As a result, and coupled with the rate of patient survey responses, the number of survey returns for the PCU are very low (Q1: n=3). The ONC unit did have this limitation and is more suitable for consideration.
SHM Converge 2023 Discussion
Our novel methods created transparency and accountability, which helped us standardize and streamline our practice of hospital medicine.
Significant insights into both unit’s day-to-day frontline care delivery were apparent. The units continue to cope with significant levels of float pool and agency nurses to provide cover, due to wider staffing and recruitment issues.
This is, unfortunately, a common cause for safety concerns in many hospitals and a knock-on effect of the impact of COVID-19 on nurse retention. Yet, this only reinforces the need for standardized care practices to cope with migratory staff who are unfamiliar with units norms and can at times exhibit less of a sense of ownership or accountability to unit performance and outcomes than fulltime staff.
Float/agency nurses must adapt to a new rounding process and delivery of patient information that can be challenging without experience. While staff are oriented to the process when on shift and given a SIBR nurse prep sheet to help them prepare, there is still an element of content delivery that requires practice and some coaching to get to a high-quality. While some staff are ‘born to SIBR’, many require coaching and feedback.
“For SIBR on this day we had all floats from the CCU (critical care unit, who had not launched SIBR at this stage), so we had to run through the SIBR structure and what their role is. It did go well even though some have never done it.”
– SIBR Rounds Manager
The oncology unit has become the de facto “practice unit” for hospitalists from other units to gain experience in SIBR, prior to launching on their own units. Two additional units have launched SIBR with 3 more planning to launch in spring/summer 2023.
As a consequence, 7 hospitalists have worked and gained SIBR experience on the ONC unit, versus only 2 new hospitalists on the PCU. With each new hospitalist starting SIBR, there is a learning curve to overcome that can cause a drop in performance. This will reduce in time as more hospitalist units begin SIBR and a general fluency with the process develops.
Patients on the SIBR units know what time SIBR rounds will occur, and where possible the team will call a designated primary carer. Restricted hospital visiting hours currently limit onsite family participation in SIBR, which may be revised in the future.
Team rounds data continues to be collected and utilized as part of the weekly unit leadership meetings to manage performance.
We believe that any clinical program seeking to improve outcomes and streamline physician workflow, interprofessional communication would likely benefit from the methods adopted as a process to standardize their hospitalist care delivery.
Leadership quotes
The Joint Commission visited us last week and asked us what we are doing to improve interdisciplinary communication. We talked all about SIBR, and they absolutely loved it.
– VP Quality
SHM Converge 2023 Conclusion
We sought to standardize our hospitalist model through implementation of the ACU care model with SIBR rounds. We have successfully implemented on two units, with an additional two units also fully launched and three more planned for the coming months.
Daily rounds quantity and quality data has been collected for ~90% of the days since launch across both units. The insights provided by this data, analytics and feedback loop have ensured a more consistent high-fidelity of unit performance with respect to the process key performance indicators.
Despite ongoing difficulties with nurse recruitment and consistent nurse staffing the units have shown improvements in clinical, throughput and patient satisfaction. On days when the units have been staffed by completely unfamiliar nurses, we have still been able to deliver SIBR with reasonable efficiency and effectiveness. This demonstrates a resilience within the units and anti-fragility to extenuating circumstances that can occur in modern acute clinical care environments.
Further analysis is required as we continue to launch our ACUs with SIBR rounds.
Further Reading
Basic, D., Huynh, E., Gonzales, R. & Shanley, C., 2018. Structured interdisciplinary bedside rounds, in-hospital deaths, and new nursing home placements among older inpatients. Clinical Interventions in Aging, 2289-2294.
Basic, D., Huynh, E.T., Gonzales, R. & Shanley, C.G., 2021. Twice-Weekly Structured Interdisciplinary Bedside Rounds and Falls among Older Adult Inpatients. Journal of the American Geriatrics Society, 69, 779-784.
Cao, V., Tan, L.D., Horn, F., Bland, D., Giri, P., Maken, K., Cho, N., Scott, L., Dinh, V.A., Hidalgo, D. & Nguyen, H.B., 2018. Patient-Centered Structured Interdisciplinary Bedside Rounds in the Medical ICU. Critical Care Medicine, 46, 85-92.
Chow, M.Y., Nikolic, S., Shetty, A. & Lai, K., 2018. Structured Interdisciplinary Bedside Rounds in an Australian tertiary hospital emergency department: Patient satisfaction and staff perspectives. Emergency Medicine Australasia.
Clay-Williams, R., Plumb, J., Luscombe, G.M., Hawke, C., Dalton, H., Shannon, G. & Johnson, J., 2018. Improving Teamwork and Patient Outcomes with Daily Structured Interdisciplinary Bedside Rounds: A Multimethod Evaluation. Journal of Hospital Medicine, 13, 311-317.
Gausvik, C., Lautar, A., Goroncy, A. & Schlaudecker, J., 2017. Significant reduction in length of stay and readmission rate over 3 years on an ace unit optimized with daily structured interdisciplinary bedside rounds. Journal of the American Geriatrics Society, 65, 101.
Gausvik, C., Lautar, A., Miller, L., Pallerla, H. & Schlaudecker, J., 2015. Structured nursing communication on interdisciplinary acute care teams improves perceptions of safety, efficiency, understanding of care plan and teamwork as well as job satisfaction. Journal of multidisciplinary healthcare, 8, 33.
Jala, S., Giaccari, S., Passer, M., Bertmar, C., Day, S., Griffith, D. & Krause, M., 2019. “In Safe Hands”–A costly integrated care program with limited benefits in stroke unit care. Journal of Clinical Neuroscience, 59, 84-88.
Loertscher, L., Wang, L. & Sanders, S.S., 2021. The impact of an accountable care unit on mortality: an observational study. J Community Hosp Intern Med Perspect, 11, 554-557.
Lopez, M., Vaks, Y., Wilson, M., Mitchell, K., Lee, C., Ejike, J., Oei, G., Kaufman, D., Hambly, J. & Tinsley, C., 2019. Impacting Satisfaction, Learning, and Efficiency Through Structured Interdisciplinary Rounding in a Pediatric Intensive Care Unit: A Quality Improvement Project. Pediatric Quality & Safety, 4, e176.
Manheim, J., Harry, E. & Mastalerz, K., 2015. Portability and Success of a Clinical Microsystem Model in Improving Safety, Quality, and Cost at a Community Teaching Hospital. Hospital Medicine 2015. National Harbor, Md.: Journal of Hospital Medicine.
Schwartz, J.I., Gonzalez-Colaso, R., Gan, G., Deng, Y., Kaplan, M.H., Vakos, P.-A., Kenyon, K., Ashman, A., Sofair, A.N. & Huot, S.J., 2021. Structured interdisciplinary bedside rounds improve interprofessional communication and workplace efficiency among residents and nurses on an inpatient internal medicine unit. Journal of Interprofessional Care, 1-8.
Stein, J., Payne, C., Methvin, A., Bonsall, J.M., Chadwick, L., Clark, D., Castle, B.W., Tong, D. & Dressler, D.D., 2015. Reorganizing a hospital ward as an accountable care unit. Journal of Hospital Medicine, 10, 36-40.