Sense-making
What is sense-making?
Sense-making is a dynamic cognitive process through which individuals interpret, organize, and assign meaning to incoming information within a specific context. In healthcare settings, clinicians engage in sense-making to decipher patient symptoms, clinical findings, and diagnostic data. This ultimately guides treatment decisions and care plans. Key components of sense-making include:
- Perception: Clinicians perceive and attend to relevant cues from the patient’s history, physical examination, and diagnostic tests, filtering out extraneous information to focus on salient clinical indicators.
- Interpretation: Clinicians interpret clinical data and patterns, synthesizing disparate pieces of information to form coherent diagnostic hypotheses and treatment plans.
- Decision-Making: Clinicians make decisions based on their interpretations of clinical information, weighing the risks and benefits of various diagnostic and therapeutic options to optimize patient outcomes.
Understanding Cognitive Load
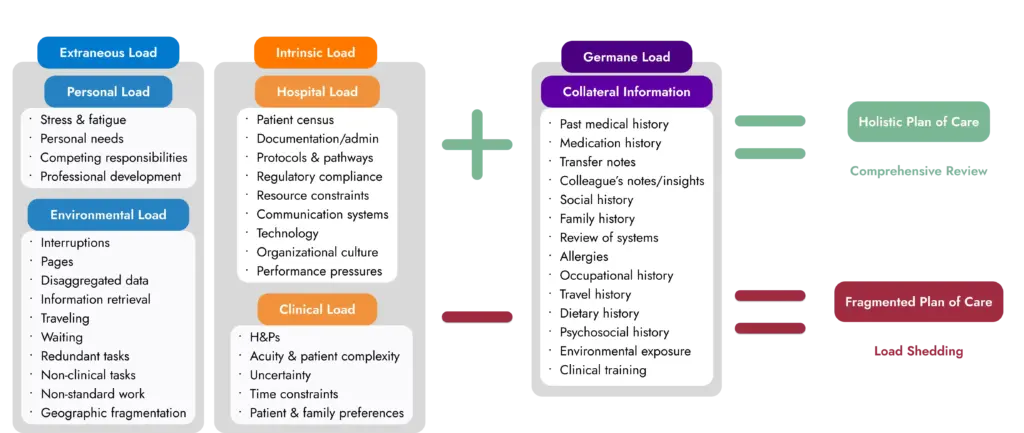
Cognitive load encompasses the total amount of mental effort required to process information and perform tasks. Cognitive load can be categorized into three main types:
Intrinsic Load
This refers to the inherent complexity of the task itself. Medical decision-making inherently involves intricate processes such as differential diagnosis and treatment selection, contributing to high intrinsic cognitive load. When assimilating and synthesizing information the number of information elements influences intrinsic load, e.g. learning about five patients co-morbidities during handover imposes more load than two1. The time available to complete a task influences intrinsic load, e.g. rapid handover and decision making for an acute patient when the Medical Emergency Team or Rapid Response Team arrive places greater load on both the sender and receiver of the information1.
Element interactivity, also increase intrinsic load1. For example, consider a patient presenting with a complex medical condition such as possible sepsis with multiple organ dysfunction syndrome (MODS). The patient’s fever, hypotension, tachycardia, altered mental status and respiratory distress could signify a variety of differential diagnoses. The physician must simultaneously consider the interplay of these symptoms and their relevance to various underlying pathologies, amplifying the intrinsic cognitive load. Additionally, the patient’s clinical history, physical exam results and diagnostic data requires extensive information synthesis, creating the potential for cognitive overload, mental fatigue and cognitive strain.
Extraneous Load
This arises from factors external to the task at hand, such as distractions, interruptions, or cumbersome documentation systems. These factors divert cognitive resources away from essential decision-making processes, impeding clinical judgment. Task-switching is a strategy to cope with what are effectively interruptions: an implicit part of clinical work2. Evidence of the burden of interruptions on cognitive load has been documented in experimental psychology and aviation, with clear associations to increased error, stress and task completion time reported. Multitasking is another common component of clinical work placing additional cognitive load on clinicians. Walter, et al. 2 analysed the impacts of task switching and multitasking on clinicians, reporting 795 task switches and 6168 multitasking instances among 17 783 tasks in total for unit based doctors, and 800 task-switches and 4482 instances of multitasking 28 809 tasks in total for unit nurses2.
Germane Load
Germane cognitive load relates to the mental effort invested in learning and understanding new information. While germane load is essential for knowledge acquisition and skill development, excessive germane load can overwhelm working memory, affecting decision-making abilities.
Clinical case conferences, grand rounds, morbidity and mortality meetings, interdisciplinary rounds all stimulate germane load for clinicians. The different specialities present, the diverse information topics discussed and the requirement to synthesize information can lead to cognitive overload.
Effects of Cognitive Load on Decision-Making
The impact of cognitive load on decision-making in healthcare is multifaceted and significant:
- Decreased Accuracy: High cognitive load diminishes the ability to process information accurately and efficiently, leading to diagnostic errors, medication mix-ups, and suboptimal treatment decisions.
- Impaired Judgment: Cognitive overload hampers clinicians’ capacity for critical thinking and reasoned judgment, increasing the likelihood of heuristic biases and cognitive shortcuts that compromise clinical decision-making.
- Reduced Adaptability: Excessive cognitive load limits clinicians’ flexibility and adaptability in response to evolving patient conditions or unexpected challenges, hindering the ability to formulate effective care plans.
- Increased Stress and Burnout: Prolonged exposure to high cognitive load contributes to elevated stress levels and emotional exhaustion among healthcare professionals, exacerbating the risk of burnout and compromising overall well-being.
Effective interdisciplinary teams engage patients and families, promote shared decision-making, offer multidisciplinary perspectives, ensure information accuracy, encourage cross-checking of data, and facilitate discussions about treatment rationale or ‘masterly inactivity.’ By embracing these components, teams can address many of the factors contributing to clinical inertia.
Optimizing healthcare to reduce the impacts of cognitive load
In healthcare, clinicians constantly juggle numerous cognitive demands, including interpreting patient data, formulating diagnoses, and devising treatment plans. Young, et al. 1 outlined the key strategies to reduce the impacts of cognitive load on clinicians:
- Strengthening the developmental intrinsic stage of the clinician, e.g. simplify the task by reducing complexity, providing more time for completion or decomposing the tasks into more manageable sections.
- Reduction of extraneous load, e.g. minimizing distractions arising from interruptions or providing information in a manner that supports cognitive focused work.
- Optimisation of germane load. Encourage the use of strategies that facilitate construction of an accurate mental model of the patient, utilize prior knowledge, compare/contrast and monitoring understanding and performance.

Strategies to Reduce Cognitive Load and Enhance Sense-Making
Hospital clinicians can employ various strategies to manage cognitive load and optimize sense-making in clinical practice:
- Streamline Information Processing: Prioritize essential clinical information and streamline documentation processes to minimize cognitive overload. Utilize structured data formats, clinical decision support tools, and electronic health record (EHR) templates to facilitate efficient information processing and decision-making.
- Enhance Information Presentation: Present patient information in a clear, concise, and organized manner to facilitate cognitive processing and decision-making. structured data formats, and standardized protocols to enhance information accessibility, comprehension and treatment response.
- Promote Situational Awareness: Foster situational awareness by maintaining a comprehensive view of the patient’s clinical status, treatment trajectory, and care goals. Encourage regular team huddles, bedside rounds, and handover discussions to facilitate information sharing and collaborative sense-making among healthcare providers.
- Implement Cognitive Offloading Techniques: Employ cognitive offloading techniques, such as checklists, algorithms, and mnemonics, to reduce cognitive burden and enhance memory retrieval. Standardize clinical workflows, protocols, and treatment algorithms to guide clinicians’ decision-making and promote consistency in care delivery.
- Enhance Team Communication: Cultivate a culture of open communication, active listening, and mutual respect among interdisciplinary team members to facilitate effective information exchange and collaborative problem-solving. Utilize communication tools such as closed-loop communication, read-backs, and situation-background-assessment-recommendation (SBAR) frameworks to enhance communication clarity and mitigate cognitive load.
Optimizing Communication Around Interdisciplinary Rounds (IDRs)
Interestingly, Manojlovich, et al. 3 found that nurse and patient participation during interdisciplinary rounds reduced interruptions and cognitive load for physicians and nurses. This was largely attributed to the communication that had taken place during rounds, with physicians commenting that the inclusion of nurses on rounds reduced the number of calls or pages and interruptions during the day. Furthermore, during IDRs nurses functioned as a reminder system for the physicians, reducing their cognitive load by reminding physicians of issues to address, that may have otherwise been forgotten.
IDRs also reduced the cognitive load for nurses: they could get the updates they needed directly from the physicians, have questions or concerns addressed, discuss orders and co-produce the plan for care and discharge. Conversely, when IDRs did not occur, and the inherent opportunity to exchange information was missed. Nurses then had to interrupt physicians more, increasing task-switching and multitasking, and their cognitive load3. Nurses also reported reduced cognitive load about patient care issues when included in team rounds.
Including patients in IDRs also reduced clinicians’ cognitive load, as they could directly participate, answering questions, providing clarifying information and potentially making decisions in the moment.
When cognitive load exceeds certain levels, we may fail to seek the inputs that may be so vital to formulating an accurate clinical picture, i.e. we load shed to prevent overload. By reducing extraneous load and making it easier to receive key collateral inputs through our SIBR rounds process, Accountable Care Units (ACUs) create information flows that free clinicians to focus on medical decision making and reduce load shedding
To explore these concepts further and discover more practical strategies for improving sense-making and integrating other advanced teamwork concepts in your teams visit our Resources.
- Young, J. Q., Wachter, R. M., ten Cate, O., O’sullivan, P. S. & Irby, D. M. Advancing the next generation of handover research and practice with cognitive load theory. BMJ Qual Saf 25, 66-70 (2016).
- Walter, S. R., Li, L., Dunsmuir, W. T. M. & Westbrook, J. I. Managing competing demands through task-switching and multitasking: a multi-setting observational study of 200 clinicians over 1000 hours. BMJ Quality & Safety 23, 231-241, doi:10.1136/bmjqs-2013-002097 (2014).
- Manojlovich, M. et al. Using Qualitative Methods to Explore Communication Practices in the Context of Patient Care Rounds on General Care Units. J. Gen. Intern. Med. 35, 839-845, doi:10.1007/s11606-019-05580-9 (2020).