In a study conducted at Wake Forest School of Medicine, the implementation of Structured Interdisciplinary Bedside Rounds (SIBR) led to a significant reduction in 7-day readmission rates, though it did not impact length of stay or 30-day readmissions.
0%
reduction in 7-day readmission rates
Objectives
To evaluate the impact of Structured Interdisciplinary Bedside Rounds (SIBR) on patient outcomes, specifically length of stay (LOS) and readmission rates, at a large academic health center.
Methods
The study was conducted over a one-year period from October 2016 to September 2017, involving 2,221 patients admitted to two hospital medicine units. One unit implemented SIBR, while the other served as a control. The SIBR team included a physician, bedside nurse, pharmacist, social worker, and bridge nurse navigator. Data were analyzed using multivariable negative binomial regression for LOS and logistic regression for readmission rates.
Results
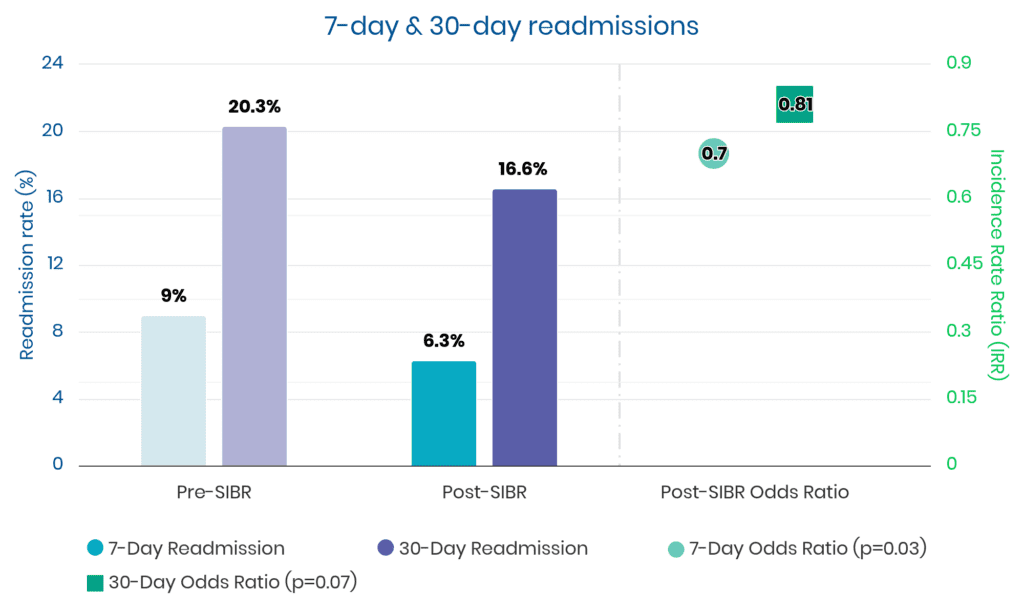
7-Day Readmission
• SIBR unit: 6.3%
• Control unit: 9.0%
• Adjusted odds ratio (OR): 0.70 (p=0.03)
30-Day Readmission
• SIBR unit: 16.6%
• Control unit: 20.3%
• Adjusted OR: 0.81 (p=0.07)
Length of Stay (LOS)
• SIBR unit: 6.7 days
• Control unit: 6.6 days
• No significant difference (p=0.58)
Conclusion
The implementation of SIBR significantly reduced 7-day readmissions, indicating an improvement in early post-discharge care. However, there was no significant impact on length of stay or 30-day readmission rates. Further research is needed to explore the potential benefits of SIBR on broader patient outcomes.
Additional Data
“We found patients admitted to the SIBR unit had similar LOS as patients admitted to the control unit and similar odds of being readmitted within 30 days of discharge. However, SIBR patients had a 30% lower odds of being readmitted within 7 days, and while the lower odds of 30-day readmission did not achieve statistical significance (p=0.07), the observed difference (19%) is clinically significant.“
I hope you enjoyed reading these strong results. Unit outcomes like these are achievable within 3 to 6 months using a seasoned implementation methodology:
skillful project management
smooth training and launch, and a
long-term partnership for sustainability.
One option to achieve similar results is to engage our 1Unit experts. Backed by 15 studies like this one, our work has received awards from The Joint Commission, CMS, Clinical Excellence Commission, IHI, BMJ, and the Society of Hospital Medicine.
Whether your unit(s) have current multidisciplinary rounds or not, our experts can guide your unit leaders to launch and sustain the best interdisciplinary teamwork and communication you’ve ever seen on a hospital ward.
This is not some ivory tower theory. Our methods have been toughened and refined worldwide. Everything we teach has been carefully tested over more than a decade, so we know it works.
Connect with us if you’d like the “Easy Button” to steadily reduce harm events, discharge delays, and patient and staff dissatisfiers.