In a study conducted at Loma Linda University Medical Center, the implementation of patient-centered structured interdisciplinary bedside rounds (PCSIBR) in the medical ICU led to increased rounding efficiency, provider satisfaction, and teaching consistency without negatively impacting patient or family perception.
0%
reduction in total rounding time
Objectives
To examine the effects of introducing patient-centered structured interdisciplinary bedside rounds (PCSIBR) in the medical ICU on rounding efficiency, provider satisfaction, and patient/family satisfaction.
Methods
The study was a prospective, nonblinded, nonrandomized, parallel group design conducted over an 8-week period from June 21, 2016, to August 15, 2016. It involved 665 patient encounters divided into PCSIBR (367) and non-SIBR (298) groups. Surveys were administered to healthcare providers (HCPs), patients, and family members to assess satisfaction and perceptions.
Results
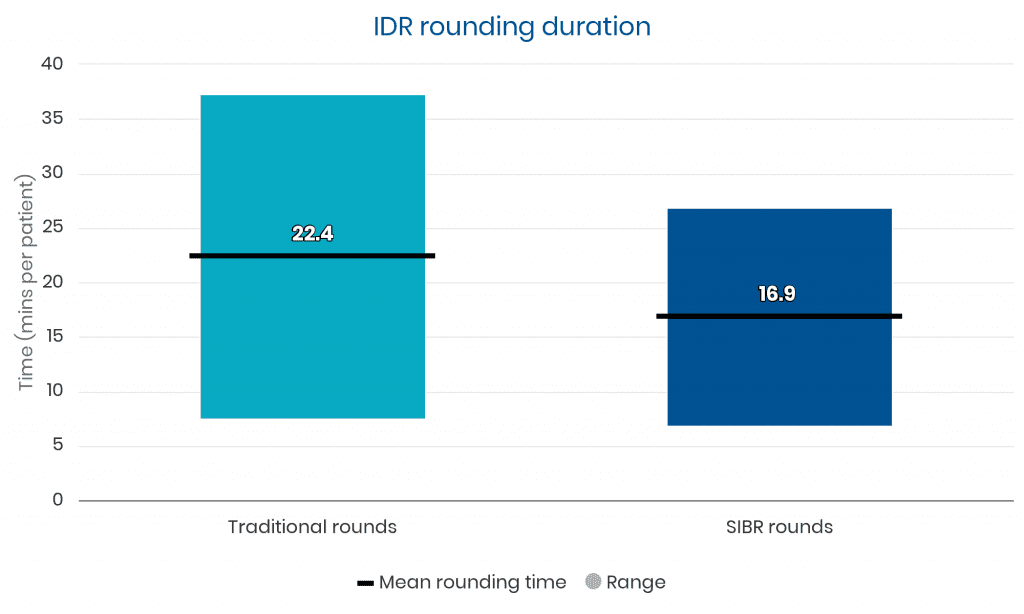
Rounding Efficiency
• Total rounding time per patient was significantly shorter with PCSIBR (16.9 ± 10.0 minutes) compared to non-SIBR (22.4 ± 14.9 minutes, p<0.01).
• Interruption time was reduced with PCSIBR (2.0 ± 2.2 minutes) compared to non-SIBR (3.9 ± 5.5 minutes, p<0.01).
Provider Satisfaction:
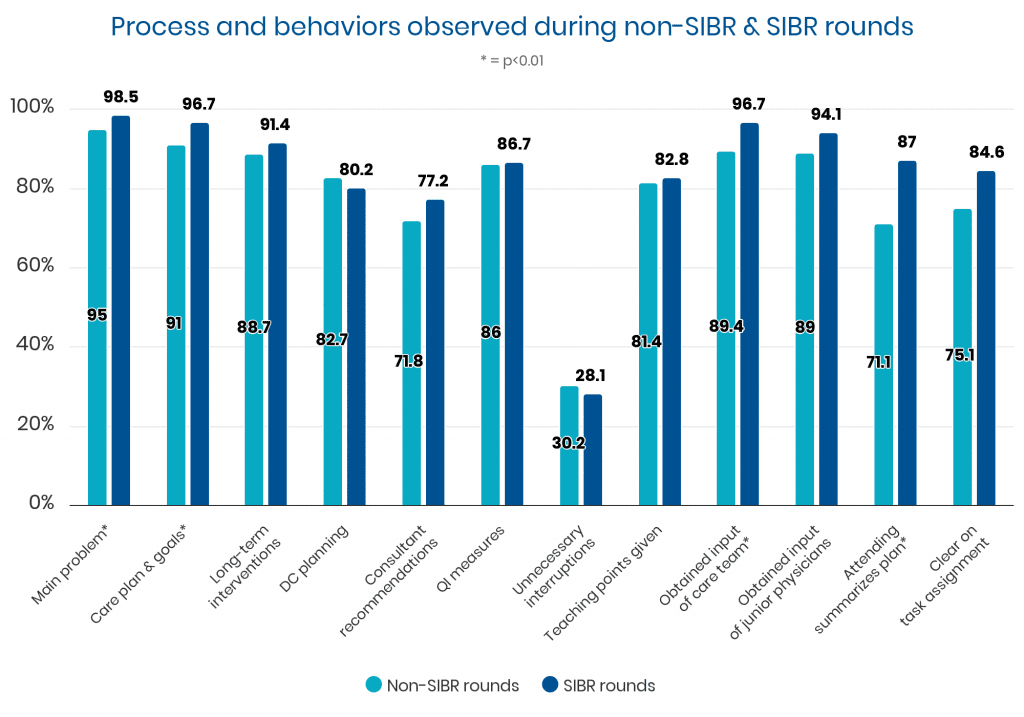
• Increased perceptions of improved communication, team input, and task clarity with PCSIBR.
• Attending physicians provided teaching points more frequently during PCSIBR (51.2%) compared to non-SIBR (33.9%, p<0.01).
Patient and Family Satisfaction:
• No significant differences in satisfaction measures between PCSIBR and non-SIBR groups.
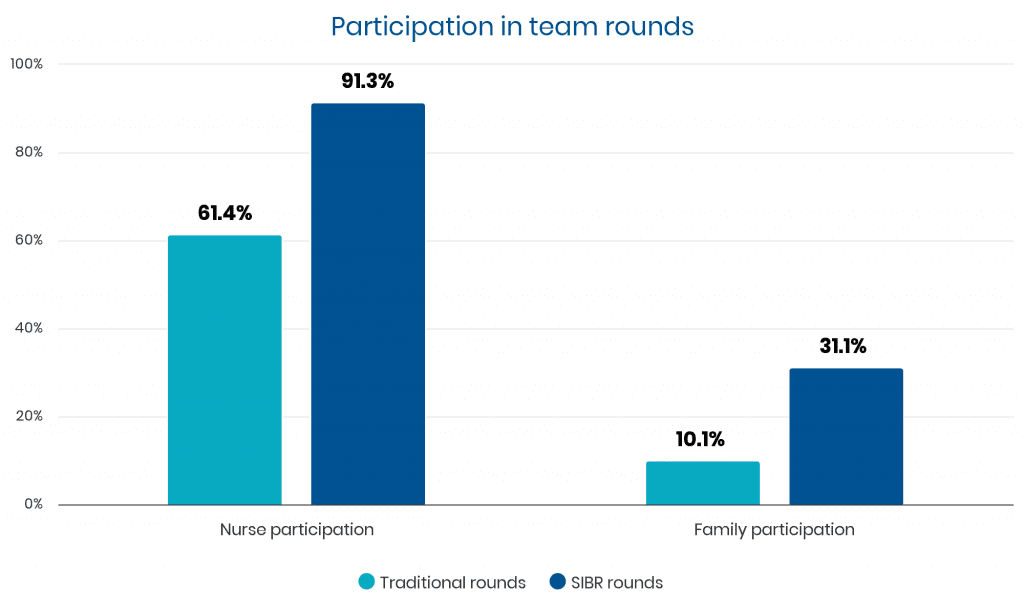
• Family presence during rounds was higher with PCSIBR (31.1%) compared to non-SIBR (10.1%, p<0.01).
Conclusion
Patient-centered structured interdisciplinary bedside rounds (PCSIBR) enhance rounding efficiency and provider satisfaction in the medical ICU without negatively impacting patient or family perceptions. This structured approach to bedside rounds improves communication, teaching, and team collaboration.
Additional Data
Rounding duration decreased an average of 5.5 minutes per patient
Evaluations of the non-SIBR rounds and SIBR rounds found that desired process elements and behaviors occurred at better rates on SIBR rounds for nearly all measures.
There was significantly higher participation on SIBR rounds than on the traditional non-SIBR rounds for nurses and family.
I hope you enjoyed reading these strong results. Unit outcomes like these are achievable within 3 to 6 months using a seasoned implementation methodology:
skillful project management
smooth training and launch, and a
long-term partnership for sustainability.
One option to achieve similar results is to engage our 1Unit experts. Backed by 15 studies like this one, our work has received awards from The Joint Commission, CMS, Clinical Excellence Commission, IHI, BMJ, and the Society of Hospital Medicine.
Whether your unit(s) have current multidisciplinary rounds or not, our experts can guide your unit leaders to launch and sustain the best interdisciplinary teamwork and communication you’ve ever seen on a hospital ward.
This is not some ivory tower theory. Our methods have been toughened and refined worldwide. Everything we teach has been carefully tested over more than a decade, so we know it works.
Connect with us if you’d like the “Easy Button” to steadily reduce harm events, discharge delays, and patient and staff dissatisfiers.