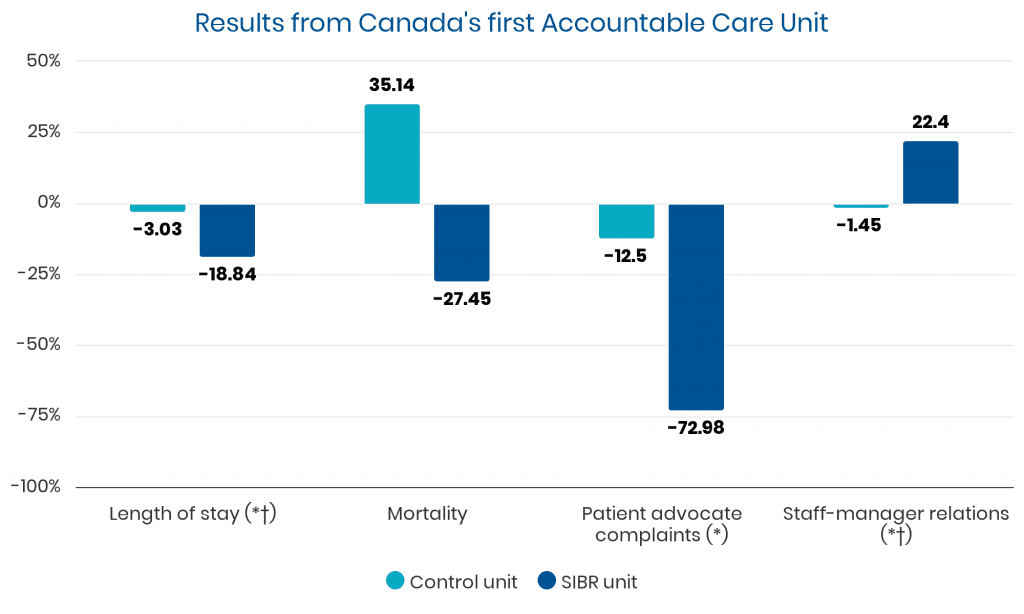
Length of Stay (LOS):
• Decreased by 18.84% (from 8.65 to 7.02 days, P<0.05) on the ACU ward.
• Control ward saw a 3% reduction (from 8.57 to 8.31 days, P=0.64).
30-Day Readmissions:
• Decreased from 15.7% to 13.3% on the ACU ward.
• Control ward decreased from 13% to 11.7%.
Mortality:
• Decreased from 5.1% to 3.7% on the ACU ward.
• Control ward saw an increase from 3.7% to 5.0%.
Patient Satisfaction:
• Significant improvements in decision making, safety, pain management, care and treatment, and patient-centered care (P<0.05).
Client Advocacy Complaints:
• Reduced from 16 to 7 on the ACU ward (P<0.05).
• Control ward saw a reduction from 16 to 14.
Staff Satisfaction:
• Improved in staff-supervisor relations (+22%) and perceptions of care provided (+17%) (P<0.05).
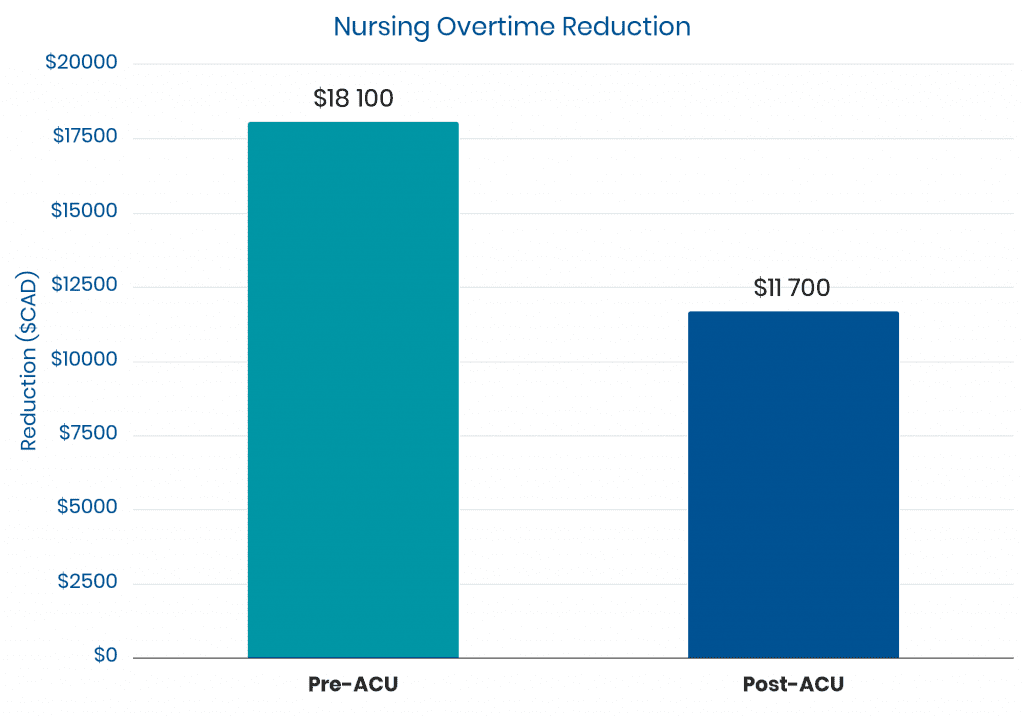
Nursing Overtime Costs:
• Decreased from $18,100 to $11,700 per month on the ACU ward.
• Control ward decreased from $17,500 to $15,300.
Process Outcomes:
• The interdisciplinary team spent an average of 51 minutes on SIBR for 14 patients per day.
• A targeted date of discharge was verbalized 97% of the time during SIBR.
Clinical Performance Outcomes:
• Improvements in documentation of VTE prophylaxis rationale, urinary catheter rationale, pneumococcal vaccination, malnutrition screening, nutritional monitoring, and patient weighing (P<0.05).