Summary: “Twice-weekly {SIBR rounds} is associated with a reduction in falls. It has the potential to be used in other settings where falls are frequent.”
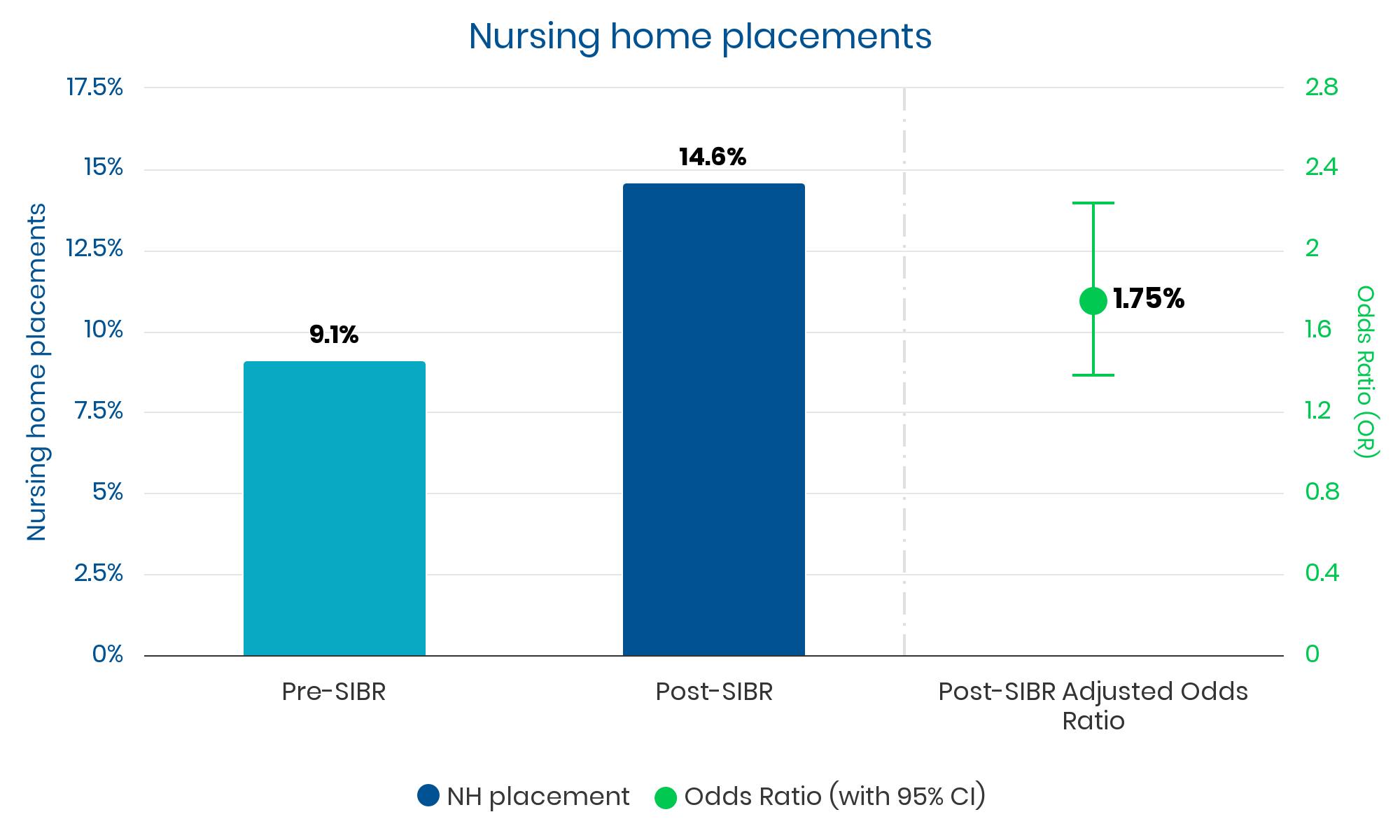
“Although the mechanisms between SIBR implementation and NH placement remain uncertain, SIBR may encourage patients and families to make decisions on placement earlier than they would have otherwise.”
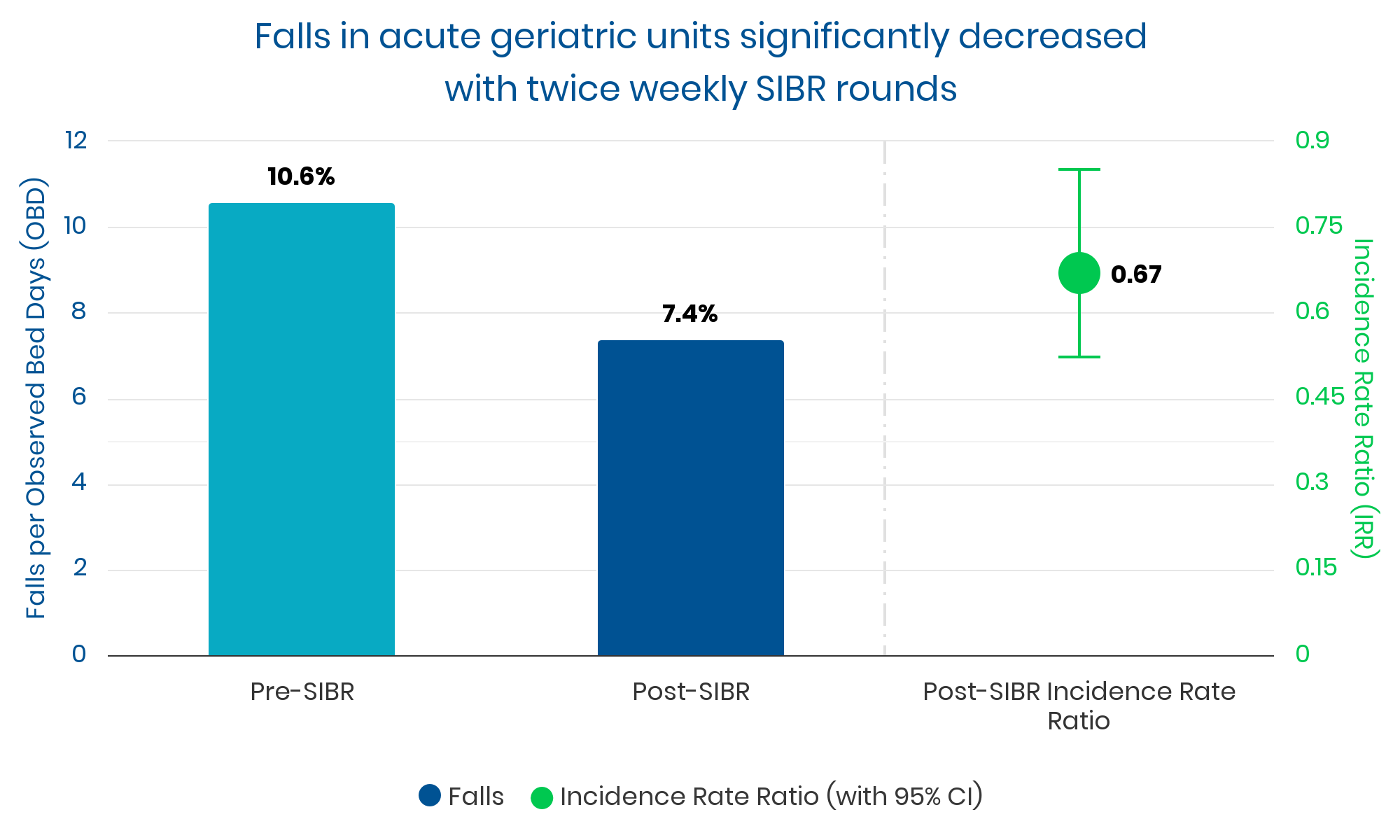
“{SIBR} incorporates a structured communication protocol and a safety checklist, which target the main risk-factors that are associated with in-hospital falls. During SIBR, each team member exchanged information that was, in many cases, directly relevant to fall risk. Relevant information that may otherwise be buried in the clinical file was rapidly communicated and addressed. …
SIBR facilitated a direct avenue for bedside nurses to communicate issues relevant to fall risk. “
Setting 2: Emergency Department, urban, tertiary hospital at Westmead Hospital.
Timeframe: SIBR implemented Nov 2012. 2 years observed (2012-2013), 1 year pre-intervention and 1 year post.
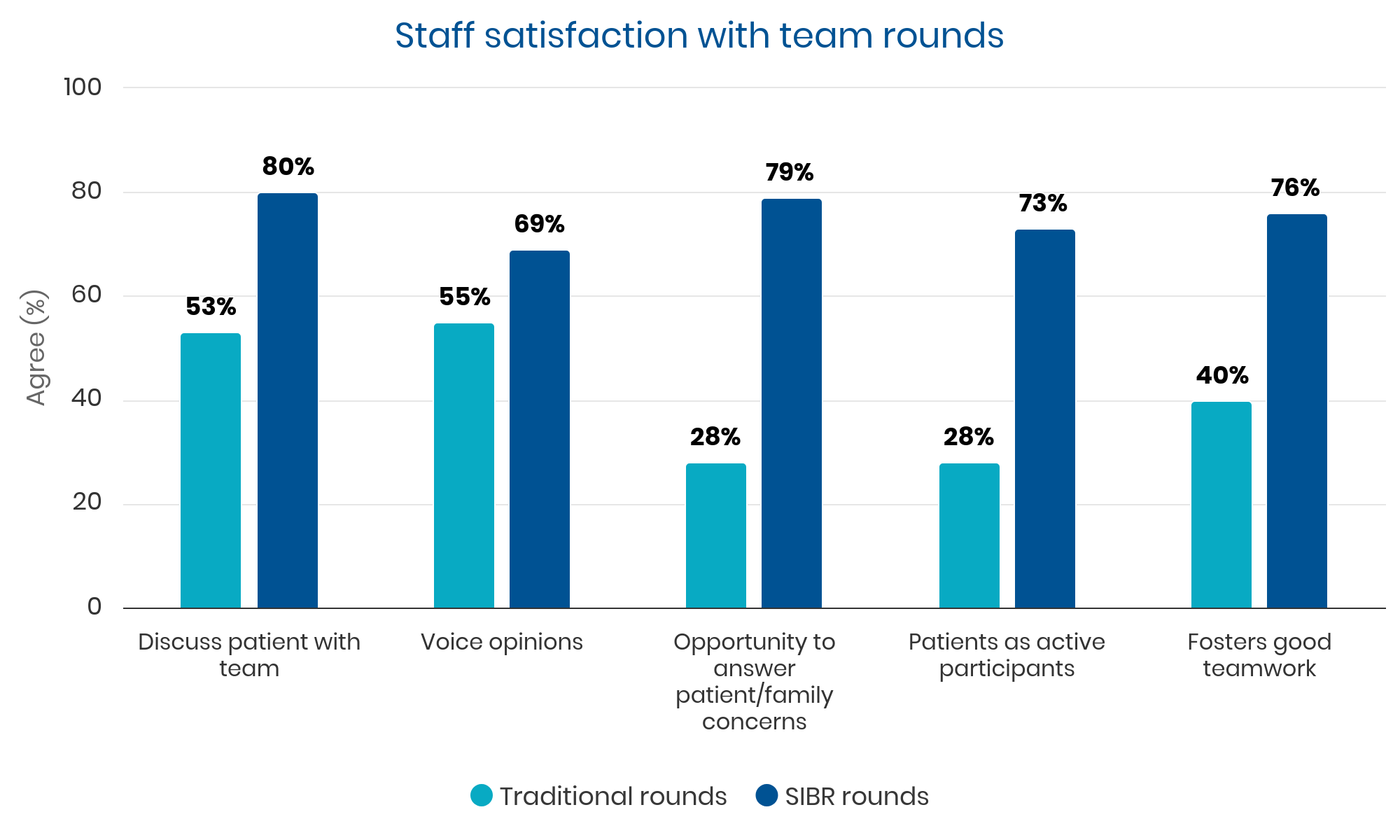
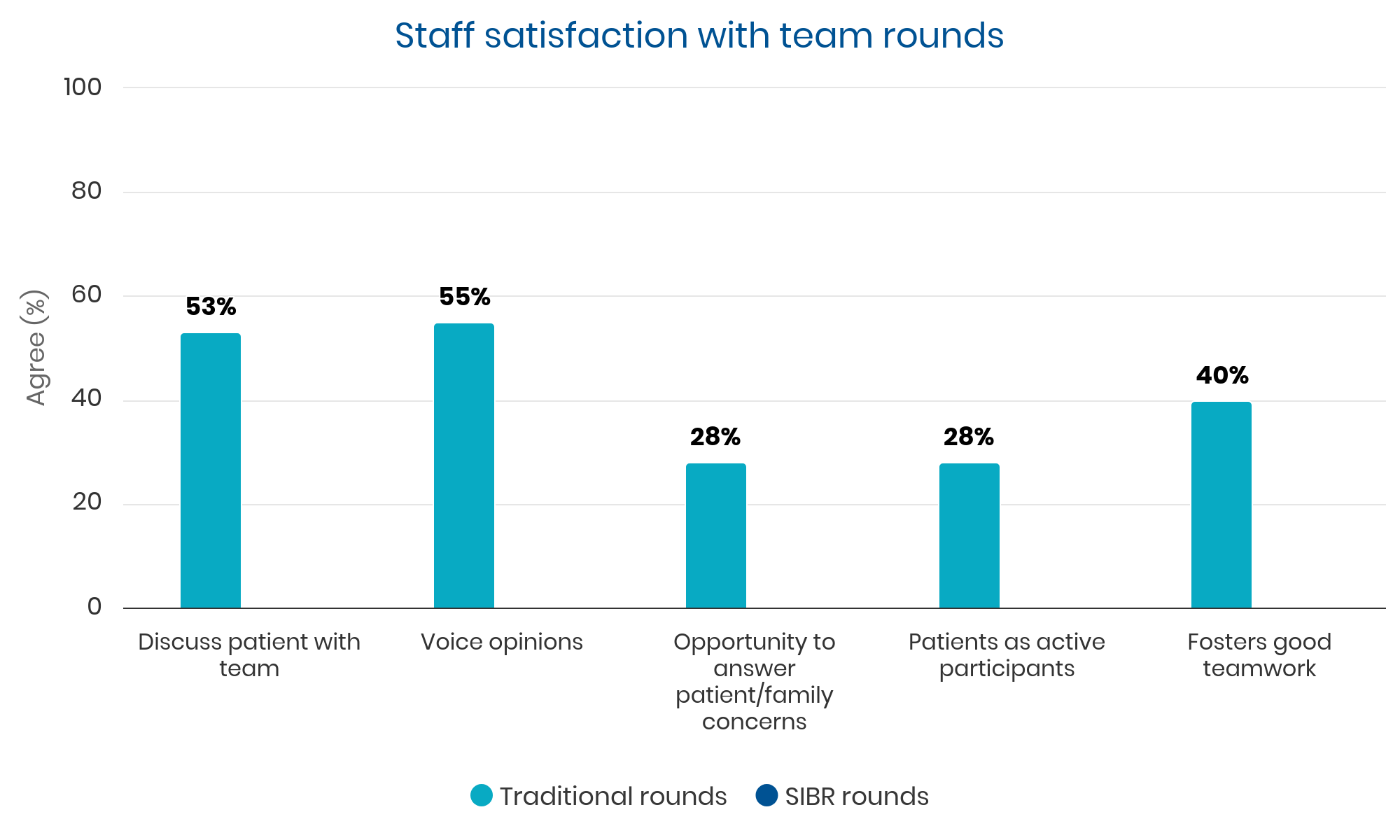
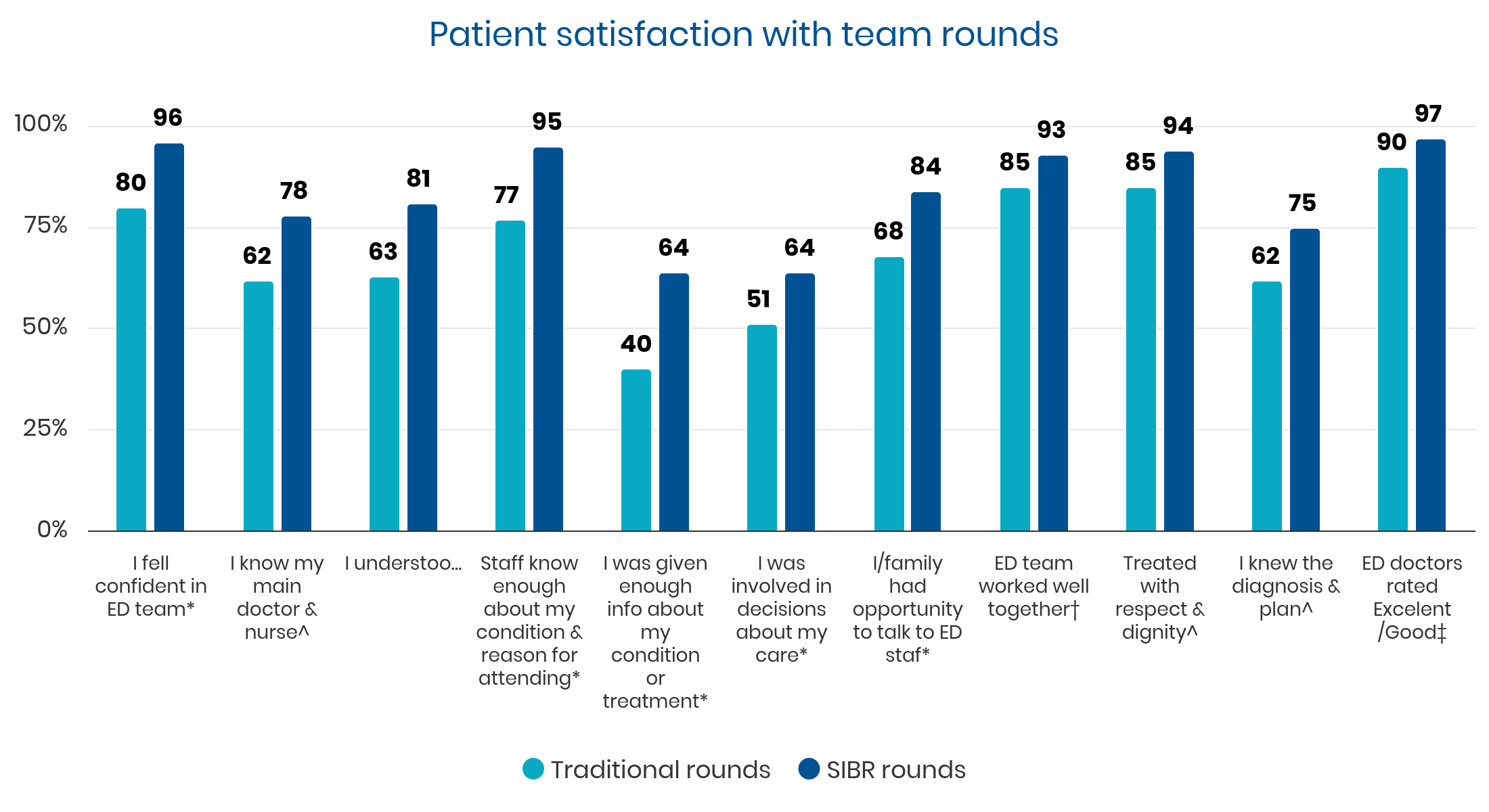
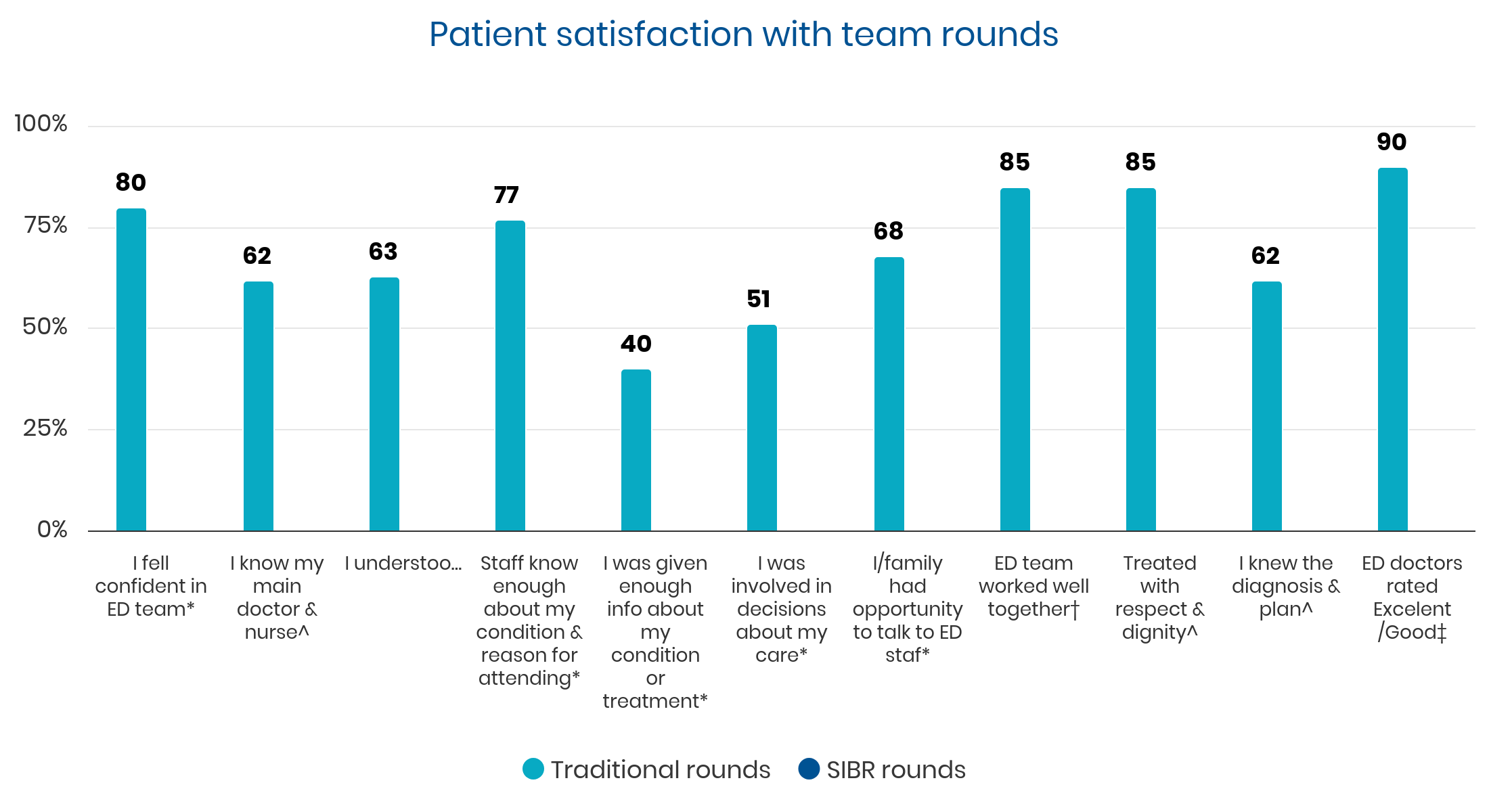
Summary: “Patient satisfaction levels towards SIBR were significantly higher than those in TR {traditional rounds}. SIBR took significantly longer time than TR per patient (122 vs 88 s). Medical staff supported SIBR in general. Challenges identified were encouragement for nursing and allied health staff involvement, the need for a flexible structure and more education.”
“This study demonstrates that patients involved in SIBR are more likely to be satisfied than those in TR {traditional rounds}. We also demonstrated that following the SIBR ward round template resulted in increased staff–patient introduction rates and patient involvement in management discussions as compared to TR.
Several respondents reported the success of SIBR ward round depended heavily on the lead senior doctor involved in the ward round. Thus we believe staff engagement, education and clinical leadership themes will need to be addressed prior to a successful implementation of such practice in other healthcare settings.”
Setting 1: Aged Care for the Elderly Unit
0%
decrease in falls with SIBR (p < 0.001)
0 IRR
(incidence rate ratio) for falls with SIBR
0%
increase in nursing home placements with SIBR
0%
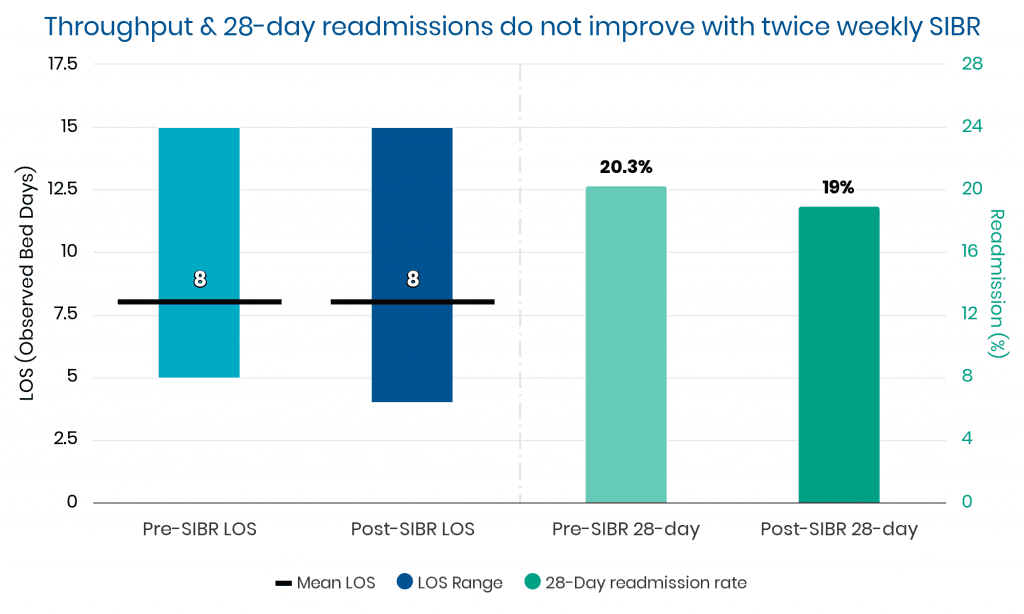
change in Length of Stay
0%
change in readmission rate
“Because of competing clinical demands, we did not believe that we could sustain daily SIBR on a long-term basis … evidence indicates that hospital discharge planning for frail older people can be improved if interdisciplinary interventions include and educate the family … only 20.3% of the SIBR in the present study were attended by a member of the family.”
Setting 2: Emergency Department
0x
increase in staff agreement that SIBR gives 'opportunity to answer patient/family concerns'
0%
increase in staff agreement that SIBR fosters good teamwork
0%
increase in patients 'I felt confident in the ED team' rating
0%
increase in patients 'Staff know enough about my condition & reason for attending' rating