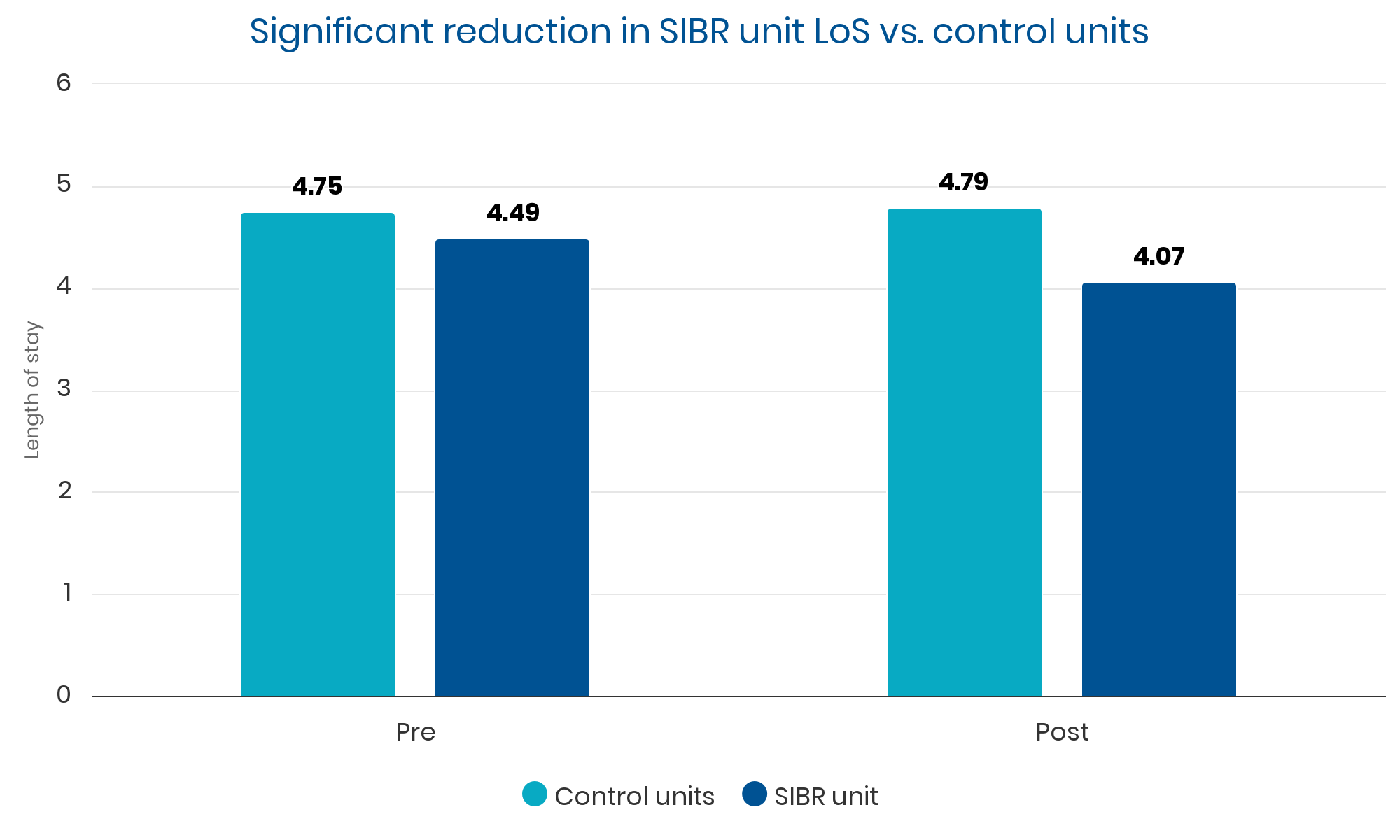
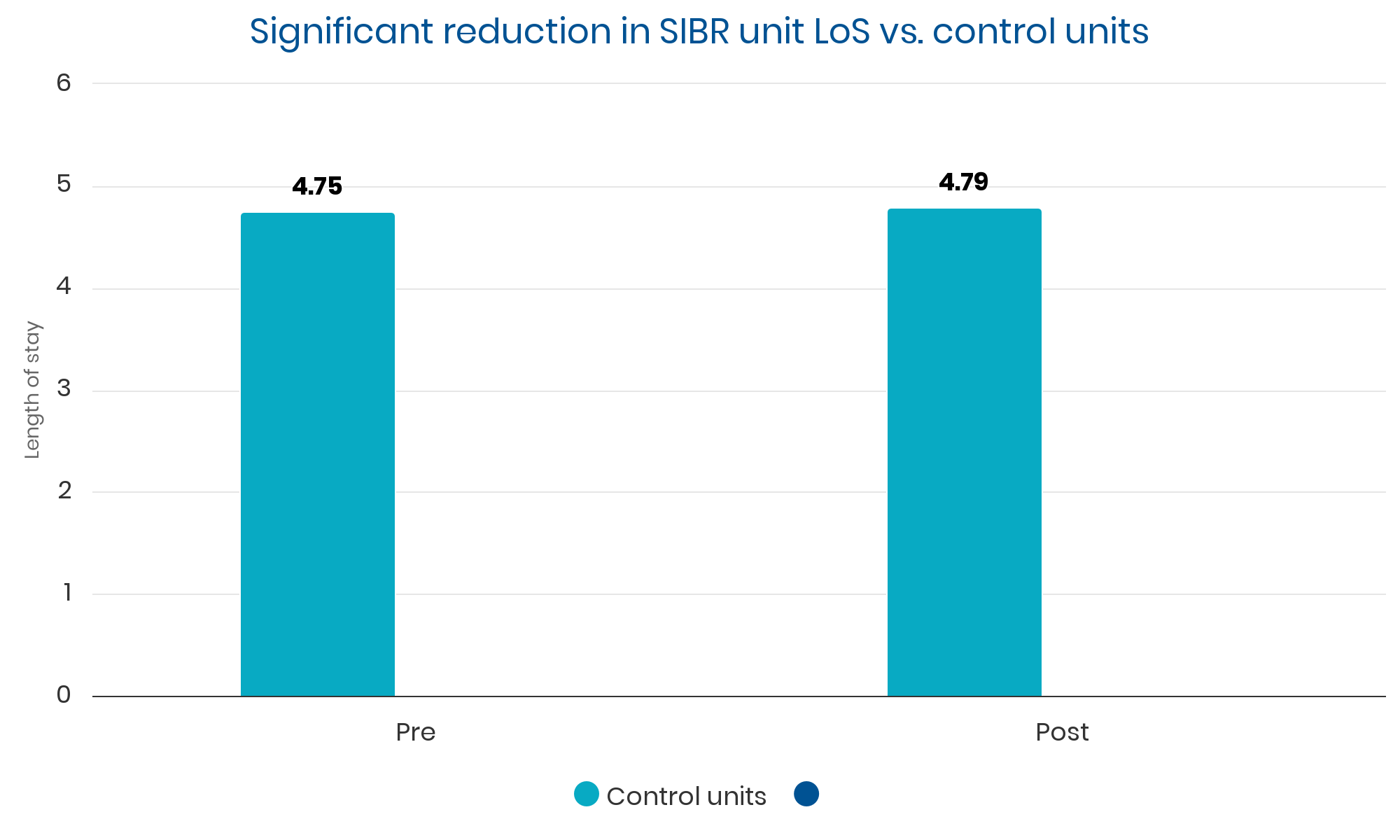
Timeframe: 21 months pre- and 21 months post-SIBR implementation
Control data: all other hospitalist groups in a 6-hospital system
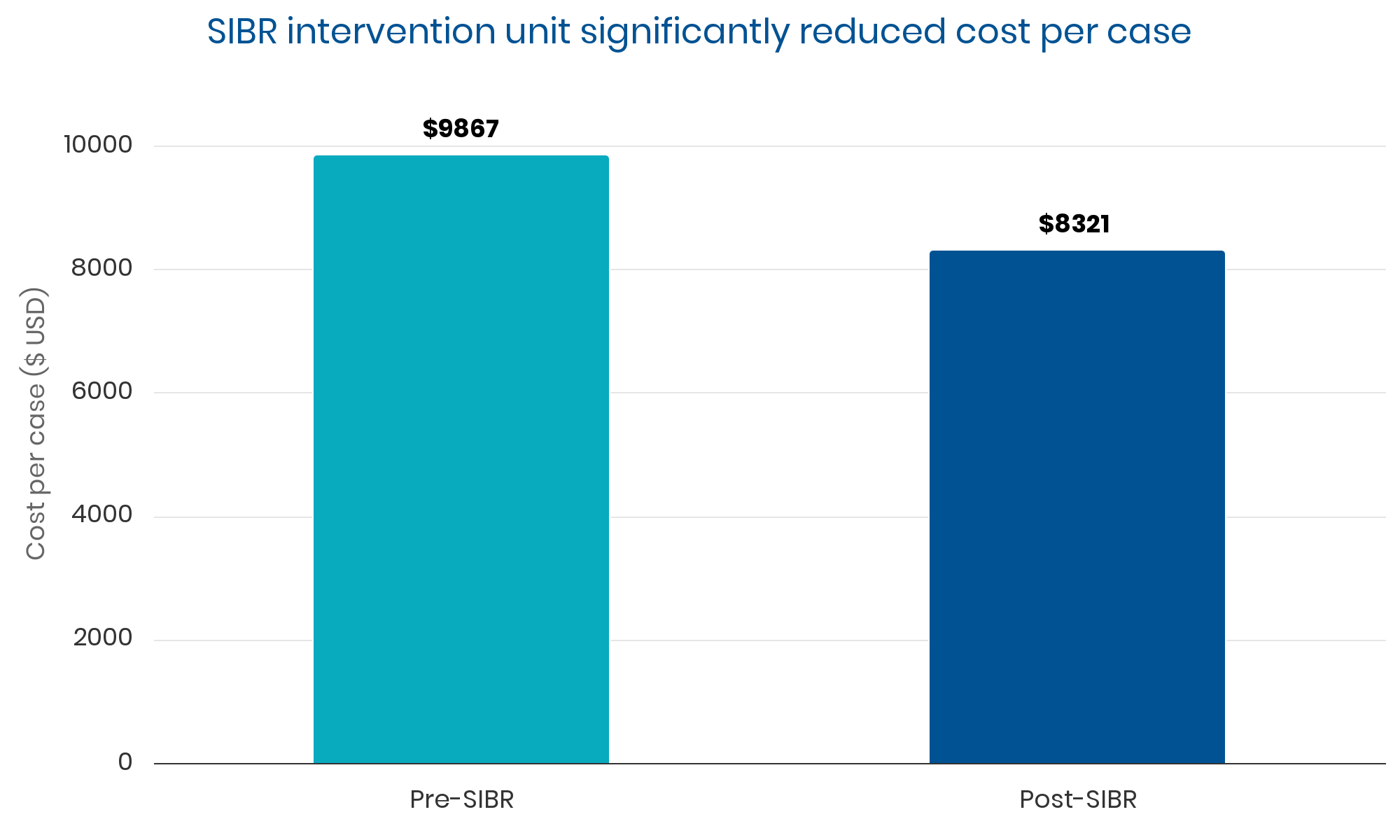
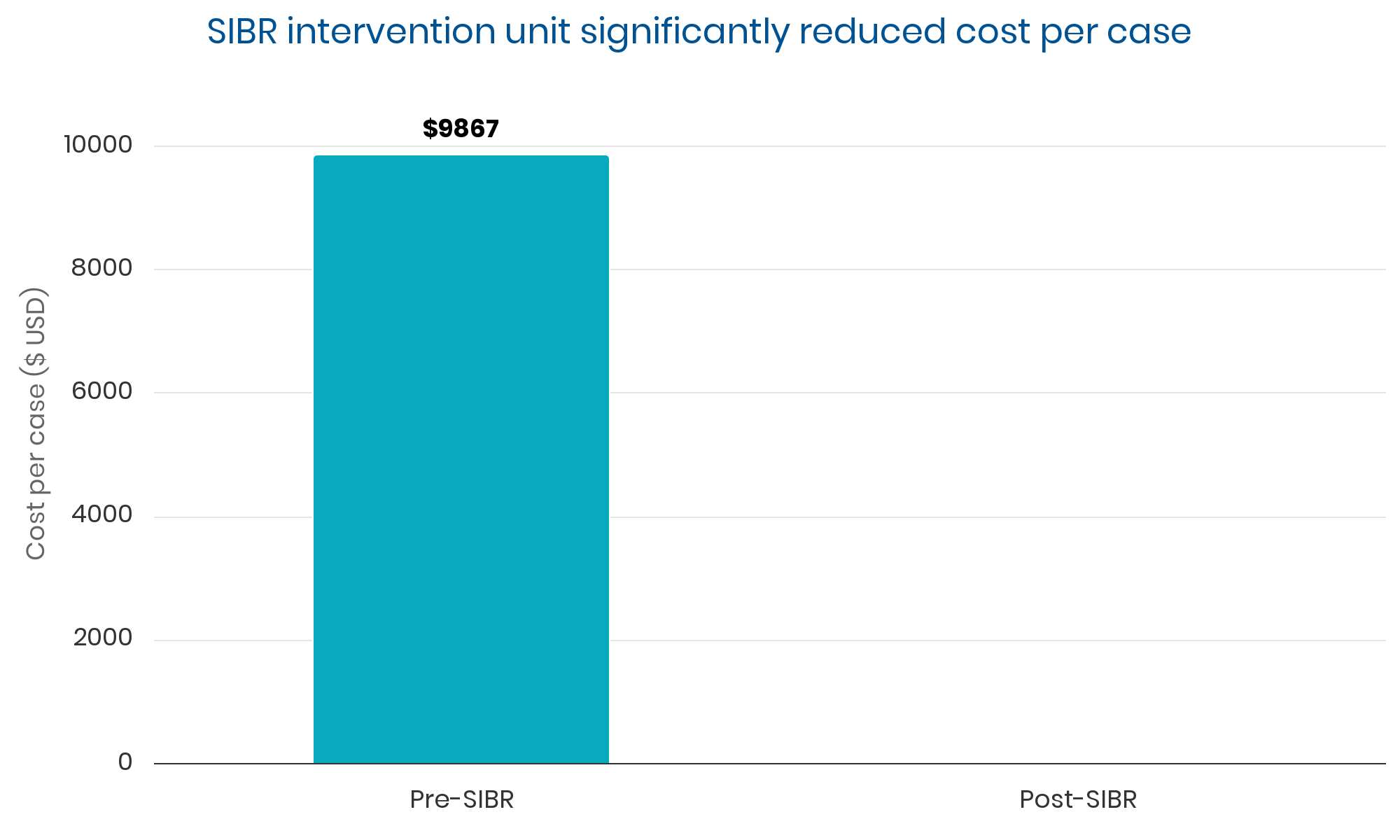
Summary: Sustained, clinically significant improvements in LOS while reducing the average cost per case. Evidence suggests these improvements were causally related to implementation of the SIBR.
“Adopters can expect to see broad quality, safety, and process improvements.”
0%
reduction in LOS (0.4 days)
0%
reduction in cost per case
$0
reduction in cost per case
$0M
savings in cost per case over 21 months
0%
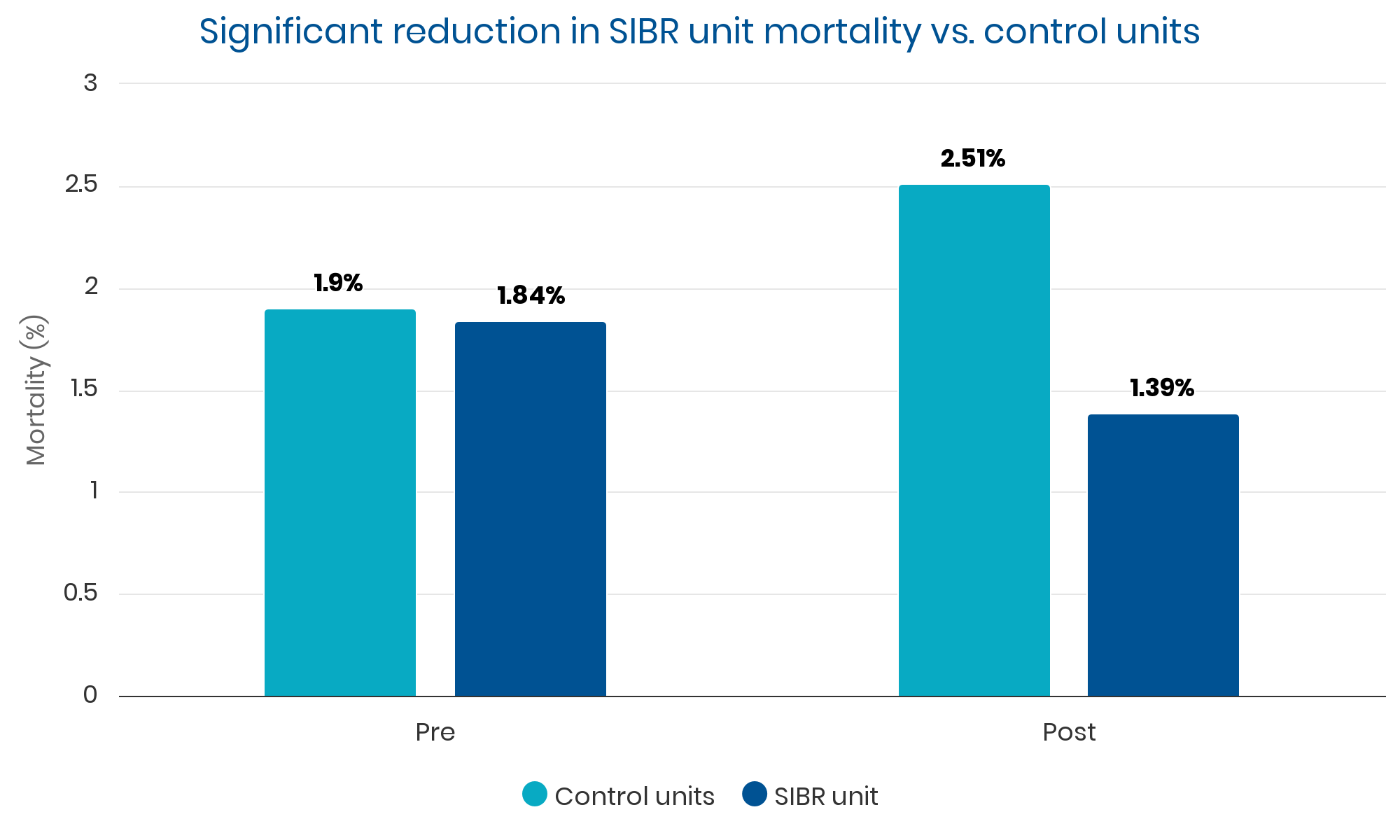
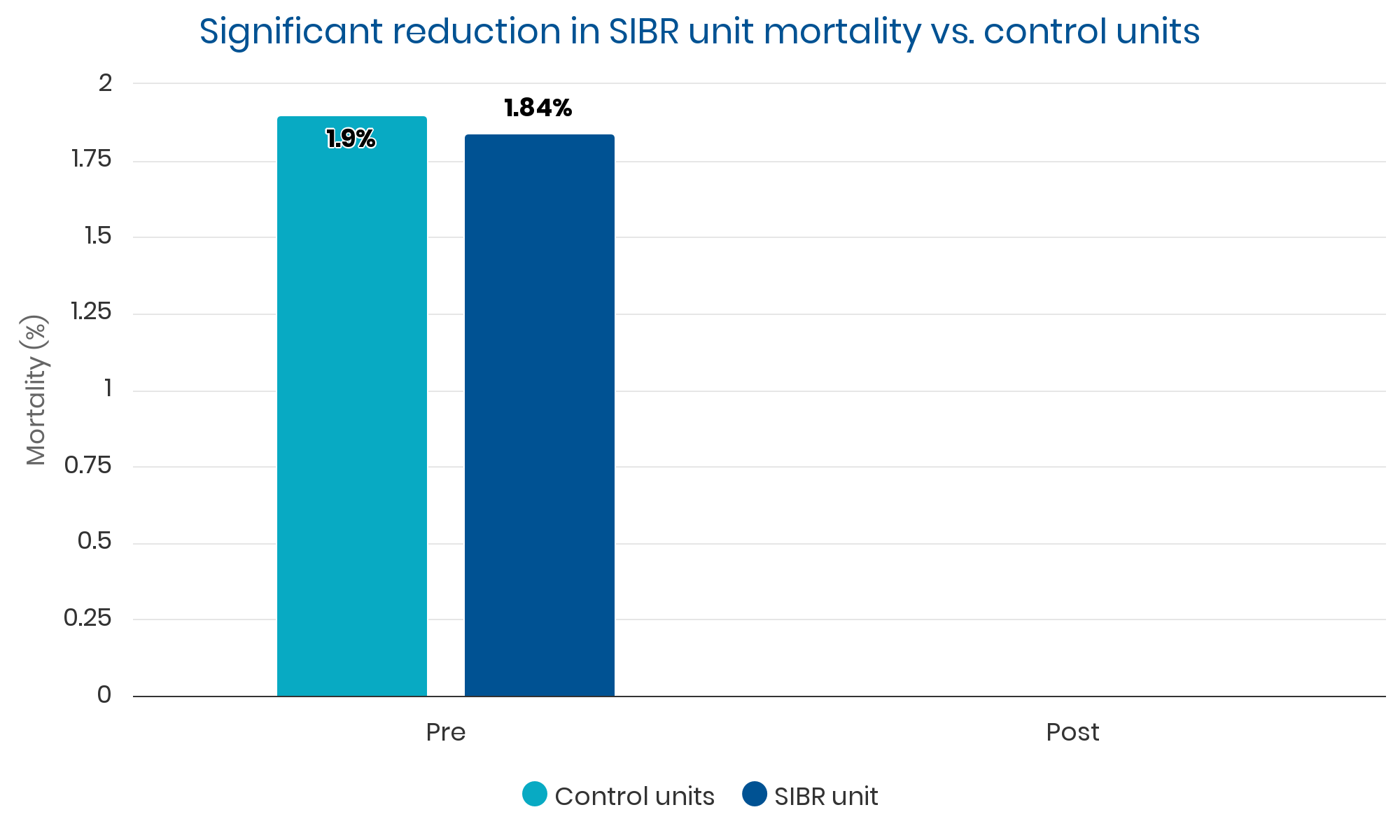
reduction in mortality
0%
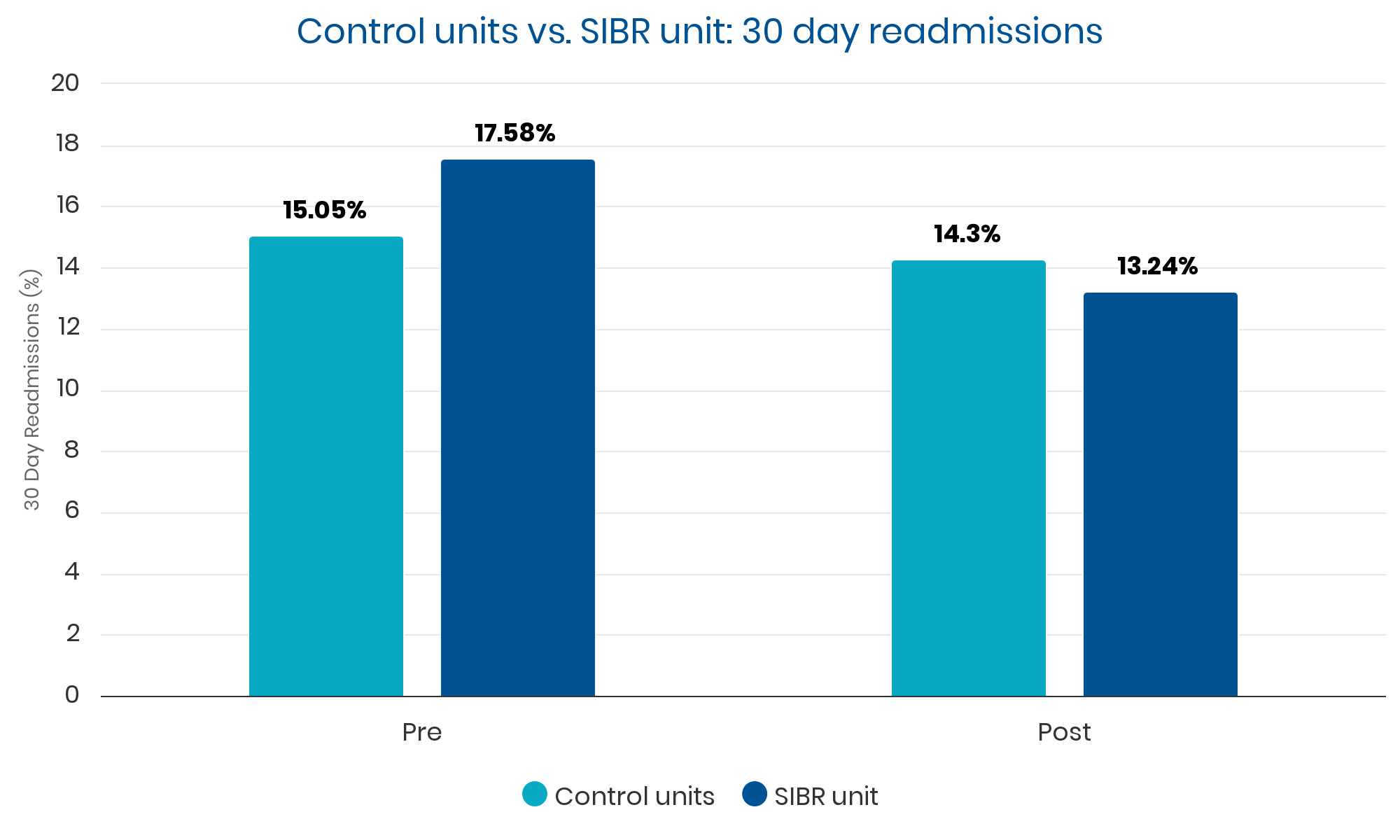
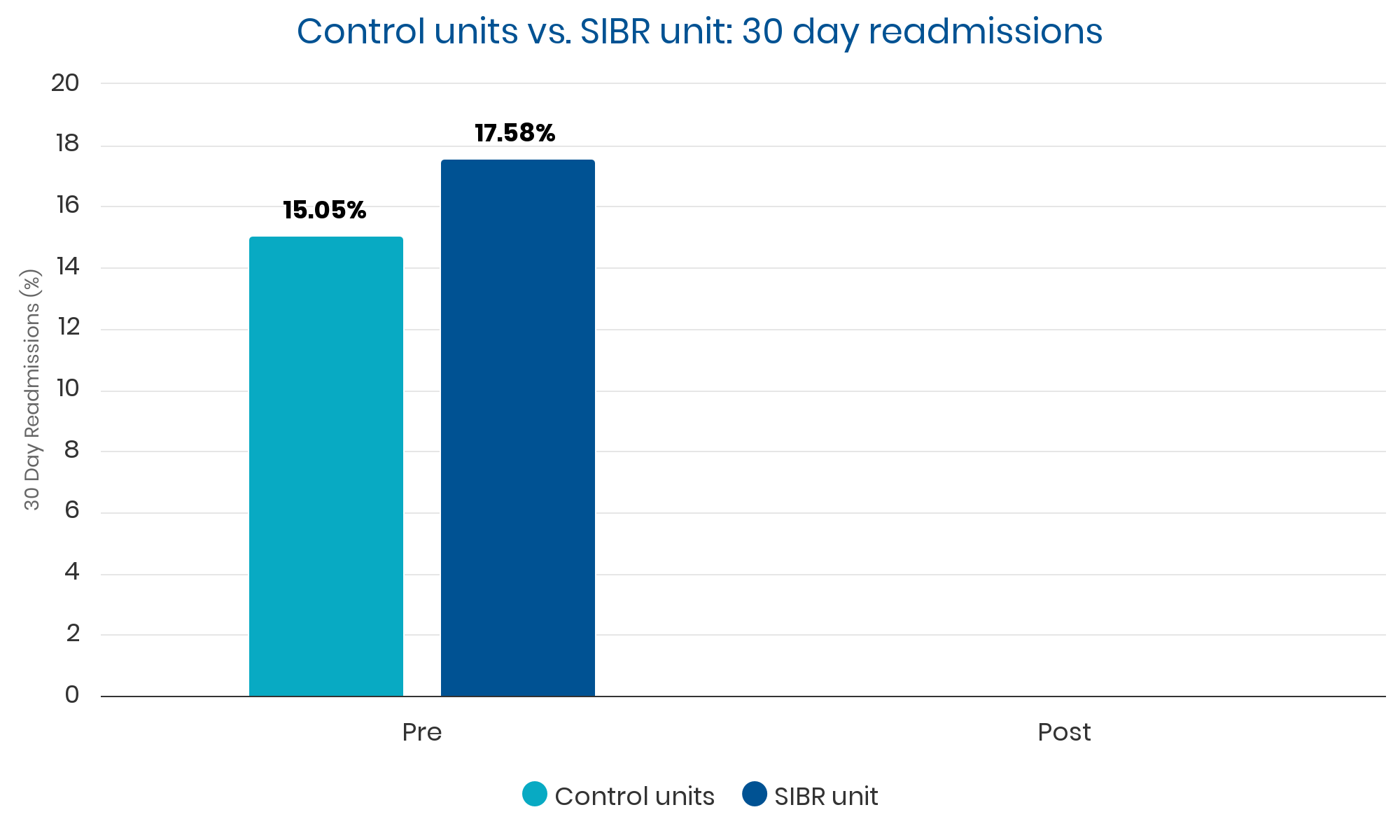
reduction in 30-day readmissions
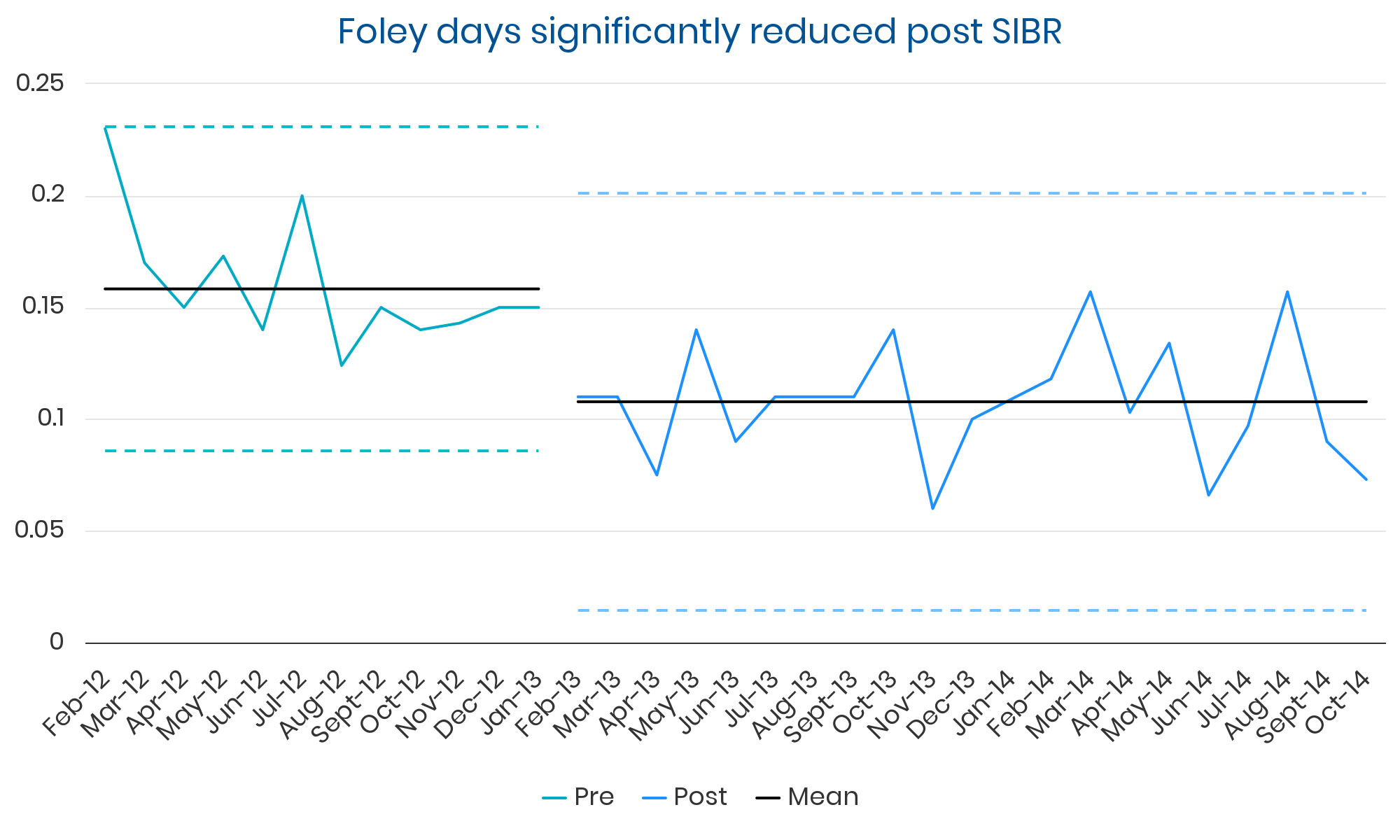
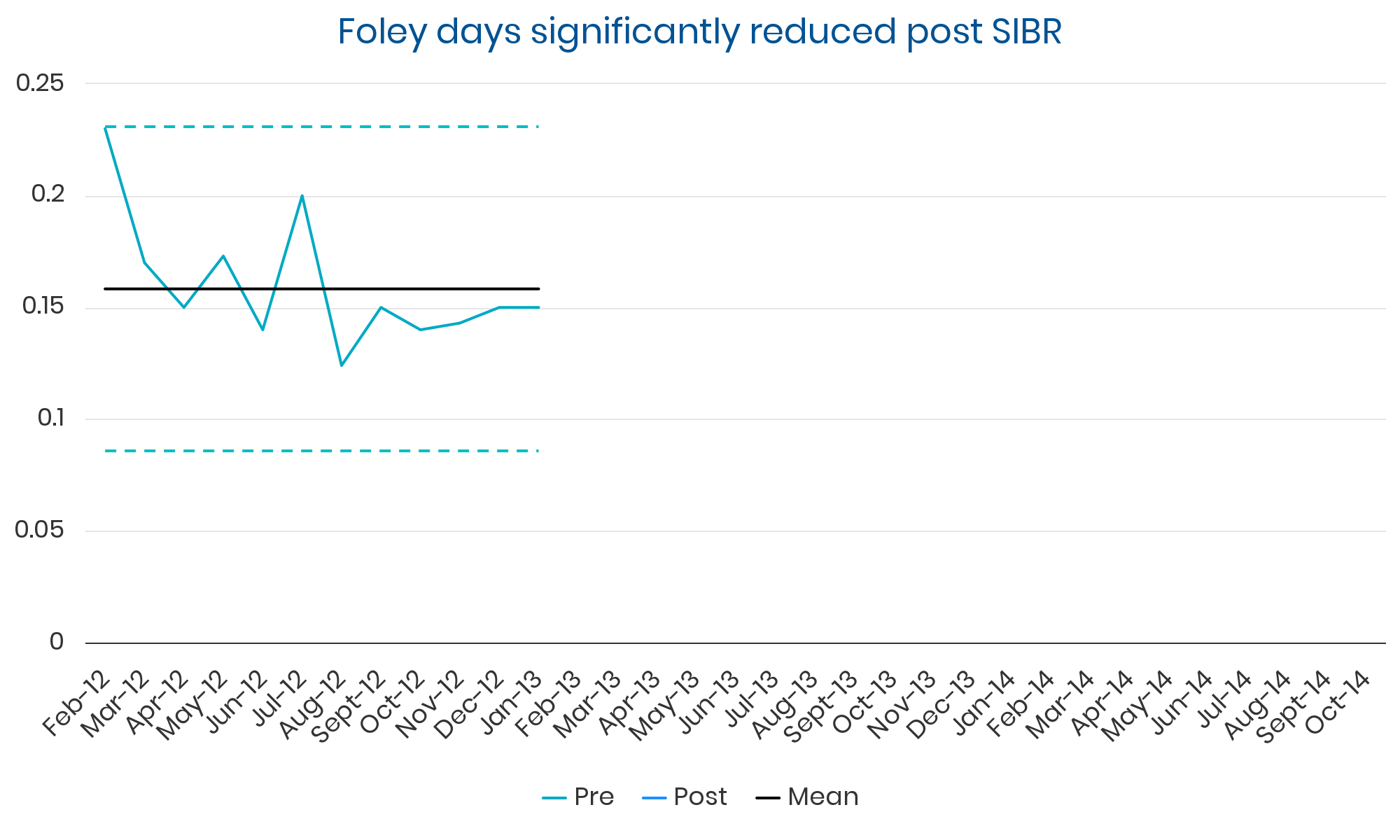
0%
reduction in average Foley days
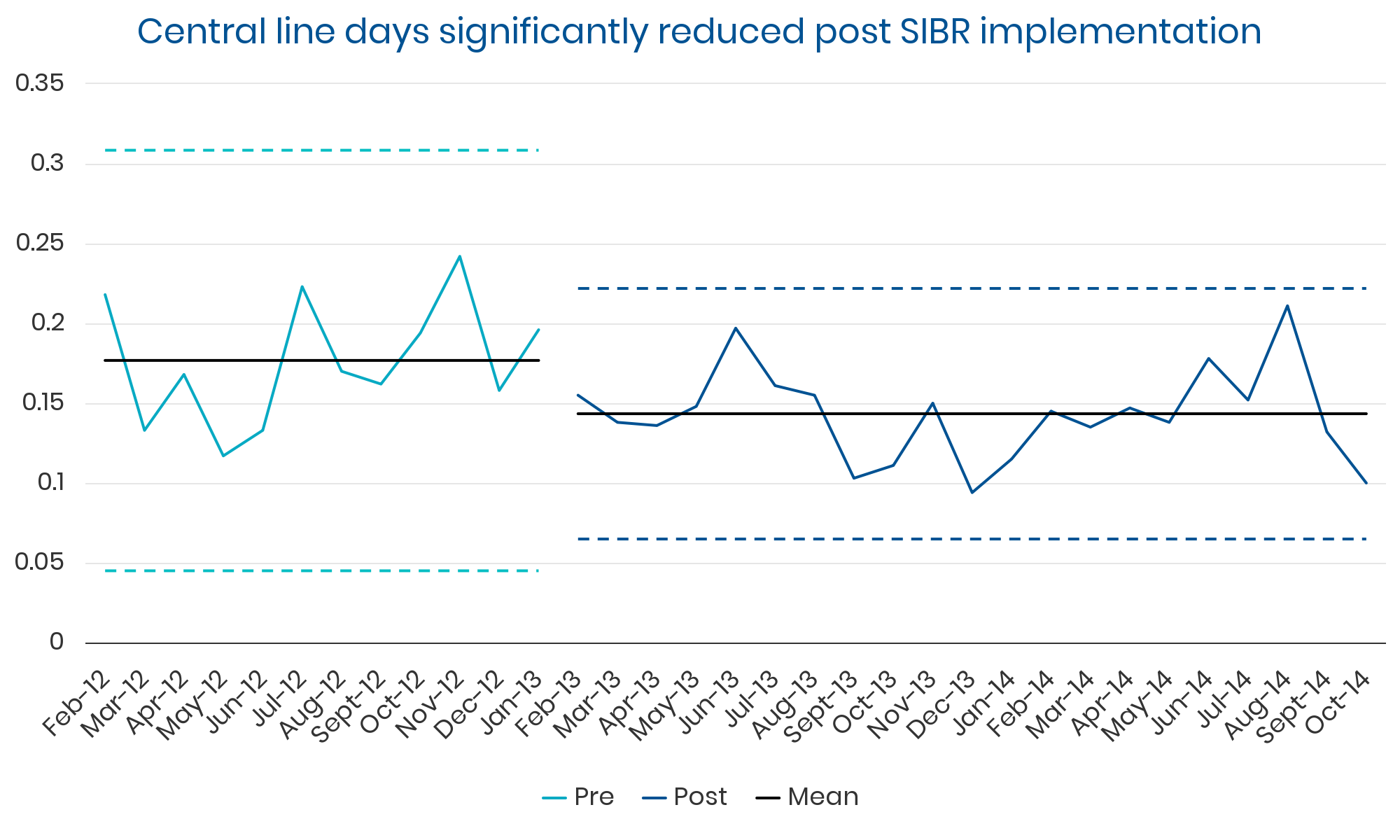
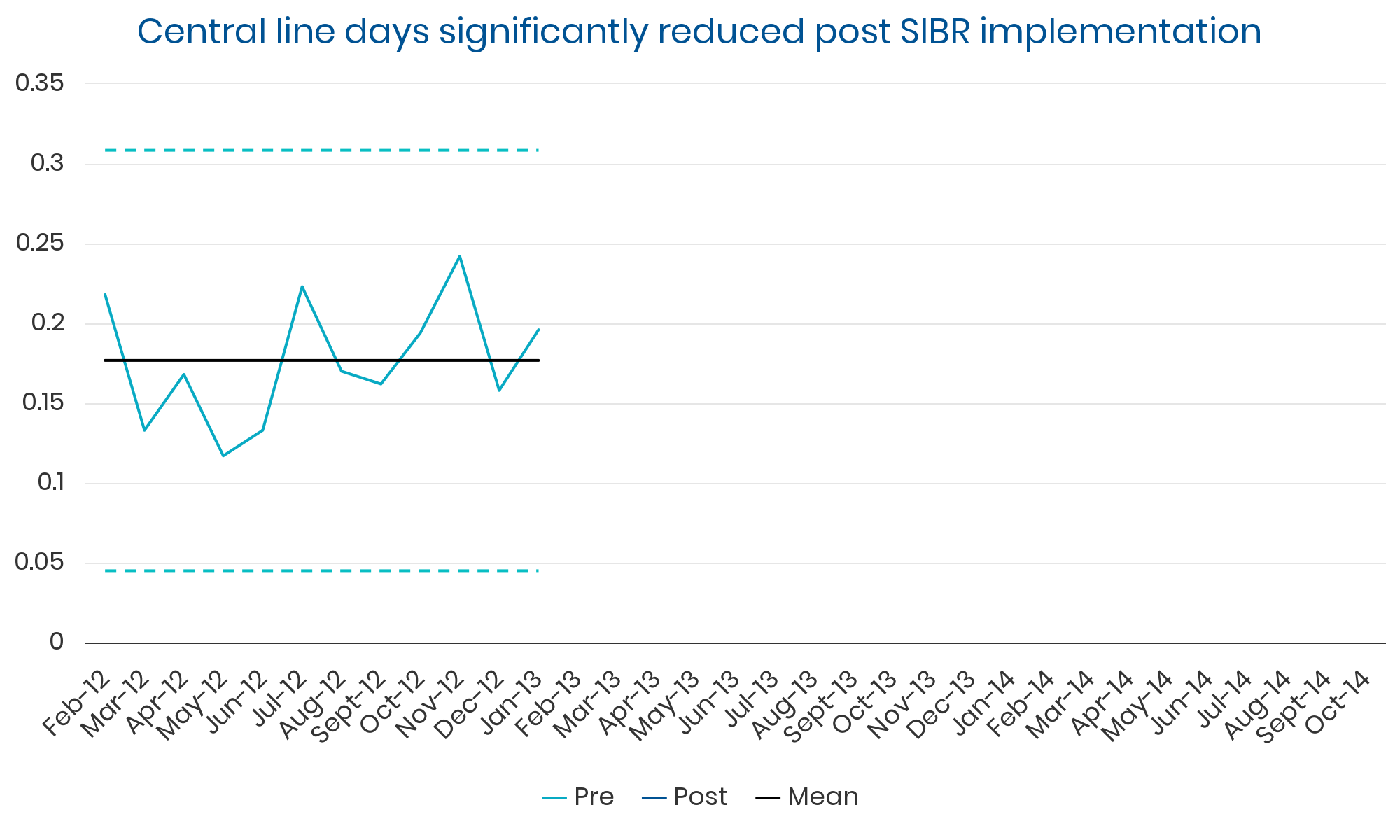
0%
reduction in average central line days
Qualitative Analysis
A subsequent qualitative analysis of the Accountable Care Units was reported, in the Journal of Hospital Medicine titled:
“We’re all truly pulling in the exact same direction”: A qualitative study of attending and resident physician impressions of structured bedside interdisciplinary rounds”.
Summary
Bedside IDR improves patient care, team collaboration, and physician empathy, but requires careful planning and stakeholder engagement.
The study of 41 resident physicians and 10 hospitalist physicians revealed five key benefits of bedside interdisciplinary rounds (IDR): reduced unnecessary care, improved risk/error screening, enhanced shared mental model of care, increased physician empathy, and streamlined communication. However, challenges included the intrusiveness of large healthcare teams and the difficulty of managing unstandardized communication in a standardized setting. To maximize the benefits of bedside IDR, leadership support and clear rounds goals are essential.
Identified Themes
Theme 1: Patient care gains from bedside IDRs
SIBR Rounds proved effective in enhancing patient care, identified by resident and attending physicians. This collaborative approach yielded several benefits, including streamlining care plans, mitigating unnecessary care, and identifying and addressing safety risks. Though some found the process occasionally resembled a performance in front of patients, they acknowledged the value in real-time input from diverse professionals, leading to improved communication, patient understanding, and overall care coordination.
“As much as I agree that it’s a show, I’m surprised how often I’m like ‘wow, going through the motions actually does help,’ where today we had a patient who was on SCDs and low molecular weight heparin and was old enough to get delirious and we didn’t even realize they still had the SCDs, so we took him off.” – (Resident 28)
“[Bedside IDR] is like a screening tool on where we’re deficient in understanding between providers. There were a couple times where we were doing discharge checklists and we had no idea how the patient was getting home.” – (Resident 27)
“One of the main advantages of multidisciplinary rounds and getting everyone on the same page is that you don’t have people calling you all day saying, ‘What’s the plan?’” – (Resident 38)c
“When you’re not in the patient’s room, you don’t have their input to correct things‐ if they’re homeless or they don’t have money, you don’t have the patient there to give you that information.” – (Attending 11)
“You learn perspective of what different teams are worried about, what they’re thinking about. They share their knowledge of something that you don’t know about every day on rounds.” – (Resident 49)
Theme 2: Increased physician empathy and
understanding
SIBR rounds improved patient care by better understanding patient priorities and fostering empathy and collaboration among the interprofessional team.
SIBR rounds allowed physicians to gather patient insights and social and emotional needs, enhancing their care approach. It also built trust and appreciation among healthcare professionals, ensuring comprehensive patient care.
Theme 3: Physician perceptions of patients'
experience of bedside rounds
The SIBR bedside IDRs led to mixed patient experiences. Positive aspects included clear communication, transparency, and reassurance. However, large teams could be overwhelming, and time constraints limited comprehensive care discussions.
“I have seen patients [saying] ‘oh wow, you guys all know each other’ and it brings a smile to their faces… they like the fact that we all are working together. It makes patients happy… it makes them trust that we’re all working on their behalf.” – (Attending 8)
“I think as a patient it could be overwhelming to have twelve people in your room at once.” – (Resident 18)
“Everyone’s concern is that it’s way less efficient. It’s this extra hour. It turns out to be the opposite, far more efficient… you probably save three hours of time on the back end for the hour up front. We still have services where we don’t [bedside IDR], where I spend hours trying to track down communication from the physical therapist.”” – (Attending 1)
“It depends on the buy‐in of other stakeholders. One pharmacist brings really helpful things to the table; [if] another pharmacist says, ‘I’m with pharmacy and we’re reviewing your meds…’ that’s not helpful.”” – (Attending 2)
Theme 4: Challenges engaging key stakeholders
One of the biggest challenges to bedside IDR was getting all relevant stakeholders involved. Staffing limitations, particularly for therapists and social workers, were a frequent issue. Physicians felt that bedside IDR was most effective when the entire team was present. However, colleagues from different professions sometimes lacked the skills or understanding required for effective participation. Additionally, both residents and attending physicians expressed concerns about the time commitment required for bedside IDR. Residents often felt that bedside IDR was an additional burden on their already busy schedules, while attendings generally found the time investment worthwhile for the efficiency it created later in the day.
Theme 5: Navigating unstandardized communication
in a standardized setting
Despite its benefits, bedside IDR posed some challenges for resident physicians. The standardized format often clashed with the patient-centered approach, and residents struggled to manage patient questions without delaying rounds or compromising other team members’ schedules. Residents also faced difficulties in navigating unstructured communication within the structured framework of bedside rounds.
“It’s difficult to balance how much you talk to the patient about their concerns during [bedside IDR] versus later on. I’ve felt that maybe other team members would’ve liked to save it for later, but I was interested in investigating it in the room with the patient. And I know people’s time is really important. I don’t know how to fix it‐ that’s a little unclear.”” – (Resident 4)
“I’ve always struggled with cutting patients off, because at the end, they instruct us to ask, ‘do you have any more questions about this plan?’ But then if they have any significant questions, you have to say, ‘sorry, we’ll come back and address that later.’” – (Resident 50)