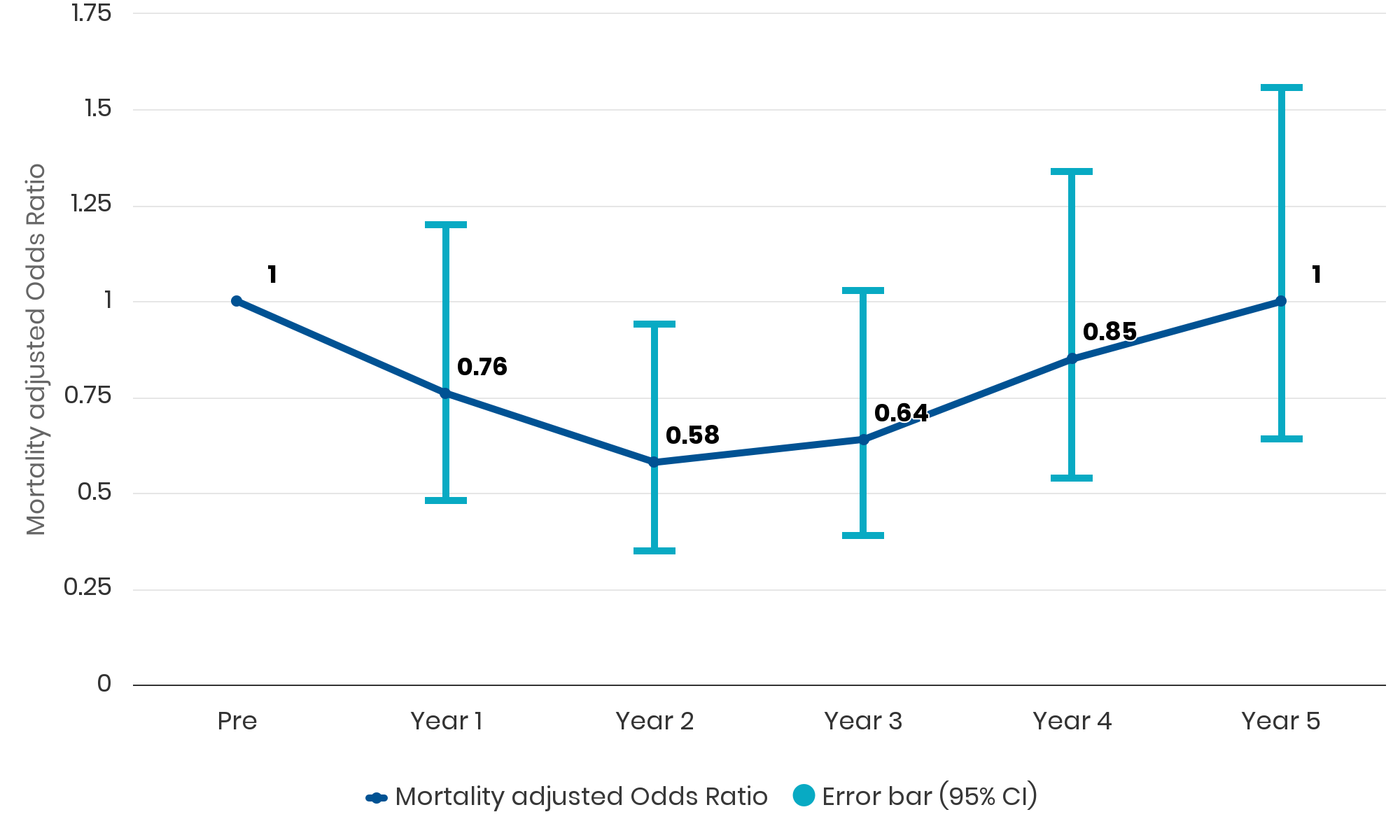
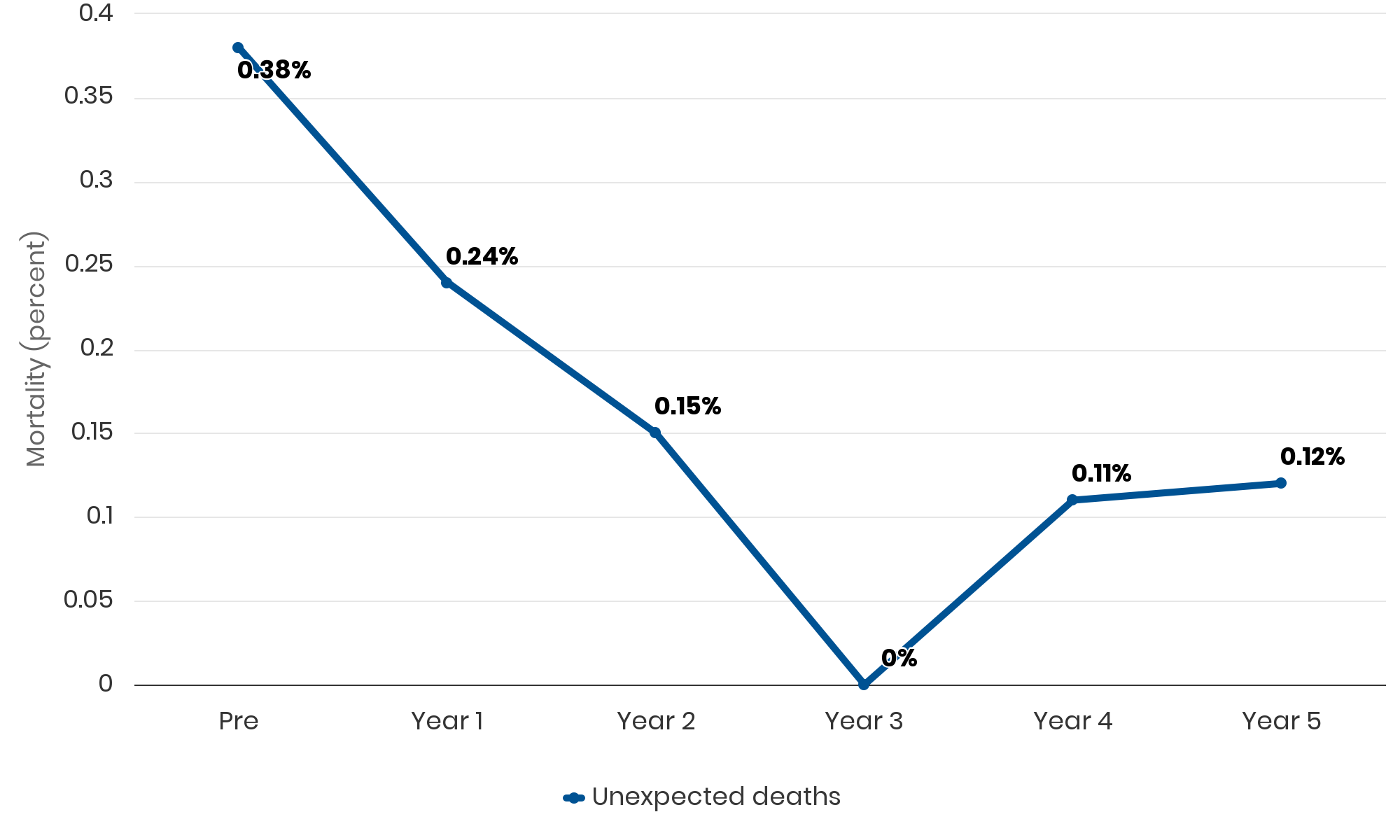
“Compared to pre-implementation year, mortality, crude or risk adjusted, showed decline in Years 1, 2 and 3, reaching statistical significance in Year 2 (risk-adjusted odds ratio [aOR] = 0.58 [0.35–0.94]). Mortality rebounded to baseline over Years 4 and 5.
In fact, early success on the ACU led hospital executives to request our help in spreading the model, diluting our focus on the original unit.“