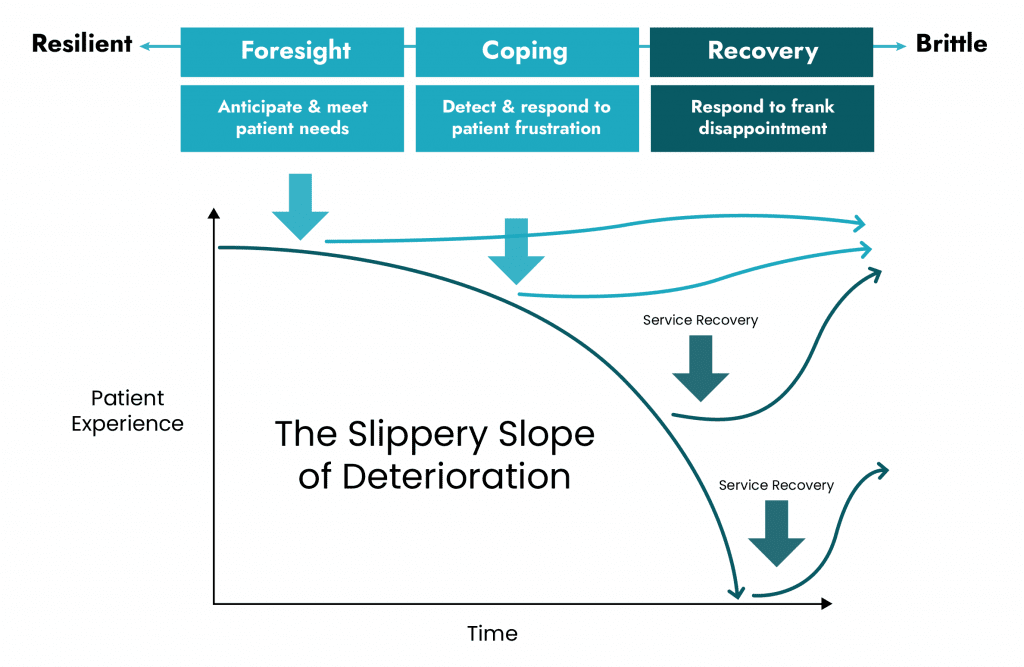
Let’s apply the concept of resilience to another scenario — a slope of deteriorating patient experience.
First, though, let’s introduce another advanced teamwork concept: cognitive empathy.
Cognitive empathy is the ability to see how a teammate — or a patient — needs help (Artman and Waern, 1998) and to take appropriate action without being asked to do so (Artman, 2000).
For teammates we show cognitive empathy by doing things that eases a physical burden (e.g., helping re-position a patient rather than standing by passively) or psychological burden (e.g., helping a teammate find 5 minutes of peace if they’re having a rough day).
For our patients we show cognitive empathy by saying or doing things that ease their frustration. Just for a minute, try thinking about patient frustration as a disease process endemic to hospitals, with predictable downward trajectory. Hospitals, after all, are places unwell people go, unhappily, to recover from a serious illness.
The etiology of frustration
The most common etiology of frustration is feeling a loss of control. The onset of frustration can be sub-acute, acute, or fulminant.
Hospital teams that fail to appreciate frustration as a disease may fail to diagnose and treat it. Detecting frustration requires specific diagnostic skills:
Active observation for eye contact, facial expressions, body language
Active listening for tone of voice, sarcasm, or frank expressions of disappointment
Active imagination for what the patient might be experiencing
Therapy for frustration should be aimed at its etiology – loss of control – with the following mainstays:
Express empathy – put the patient’s facts and feelings into a sentence so the patient feels understood [O’Neal, 2014]; helping a patient or family member feel understood is always required (and sometimes it’s even sufficient) to help manage a patient’s frustration
Offer options – find a way to re-frame even the smallest part of the patient’s circumstance, whatever it may be, as a set of choices; having choices means having a sense of control; choices can be offered in seemingly trivial circumstances (e.g. “would you like me to close the door, or leave it open?”); of course the ultimate form of control is making sure the patient is calling the shots in a way that aligns with their goals of care.
In other words, hospital teams can become proactive in managing patient satisfaction by using cognitive empathy for foresight (anticipating and meeting patient needs) and and coping (detecting and responding to frustration as soon as it arises).
To do this, great teams think differently about the patient, and still rely on each other to recognize the more subtle forms of frustration and respond appropriately.
Artman, H. & Wærn, Y., 1998. Creation and loss of cognitive empathy at an emergency control centre. In Y. Wærn (ed.) Cooperative process management: Cognition and information technology. London, UK: Taylor & Francis, 69-76.
Artman, H., 2000. Team situation assessment and information distribution. Ergonomics, 43, 1111-1128.