Our highly coordinated, patient-centered model is associated with more efficient and reduced cost of care. By utilizing Structured Interdisciplinary Bedside Rounds (SIBR® rounds) to optimize throughput, avoidable costs can be minimized or eliminated.
In addition, reducing length of hospital stays due to efficiency and faster discharge protocols increases savings to the patient and hospital.
Mechanisms of Action
SIBR rounds help to reduce direct and indirect costs by coordinating the plan for the day and discharge plan on a daily basis.
Within 3-5 minutes every participant has heard from their colleagues, the patient, and their family (if present). Everyone leaves the bedside with their key questions answered and a cohesive holistic plan for the day and plan for discharge shared amongst the team.
Early discharge planning, embedded into the SIBR 6-step communication protocol, helps to ensure patients can discharge as soon as they are medically ready. Many of the common causes of hospital acquired conditions and infections are proactively addressed by the team each day, including:
placement decisions are made earlier,
medications get down-titrated,
IV to PO orders are placed,
drips, lines and drains are removed,
mobility & deconditioning are addressed, and
pressure wounds and fall protocols get activated.
Consequently, team members, patients and family members know what their tasks are until the team meets again, and how they can each progress the patient to a safe and early discharge.
The incorporation of a quality-safety checklist into our bedside handover process and again in SIBR rounds ensures that common causes of hospital acquired complications are identified and mitigated early, 3 times per day at a minimum. This prevents non-response to treatment or deterioration that can delay patient recovery and discharge.
Get the detailed Cost Savings outcomes
All the information needed to speak confidently about the outcomes.
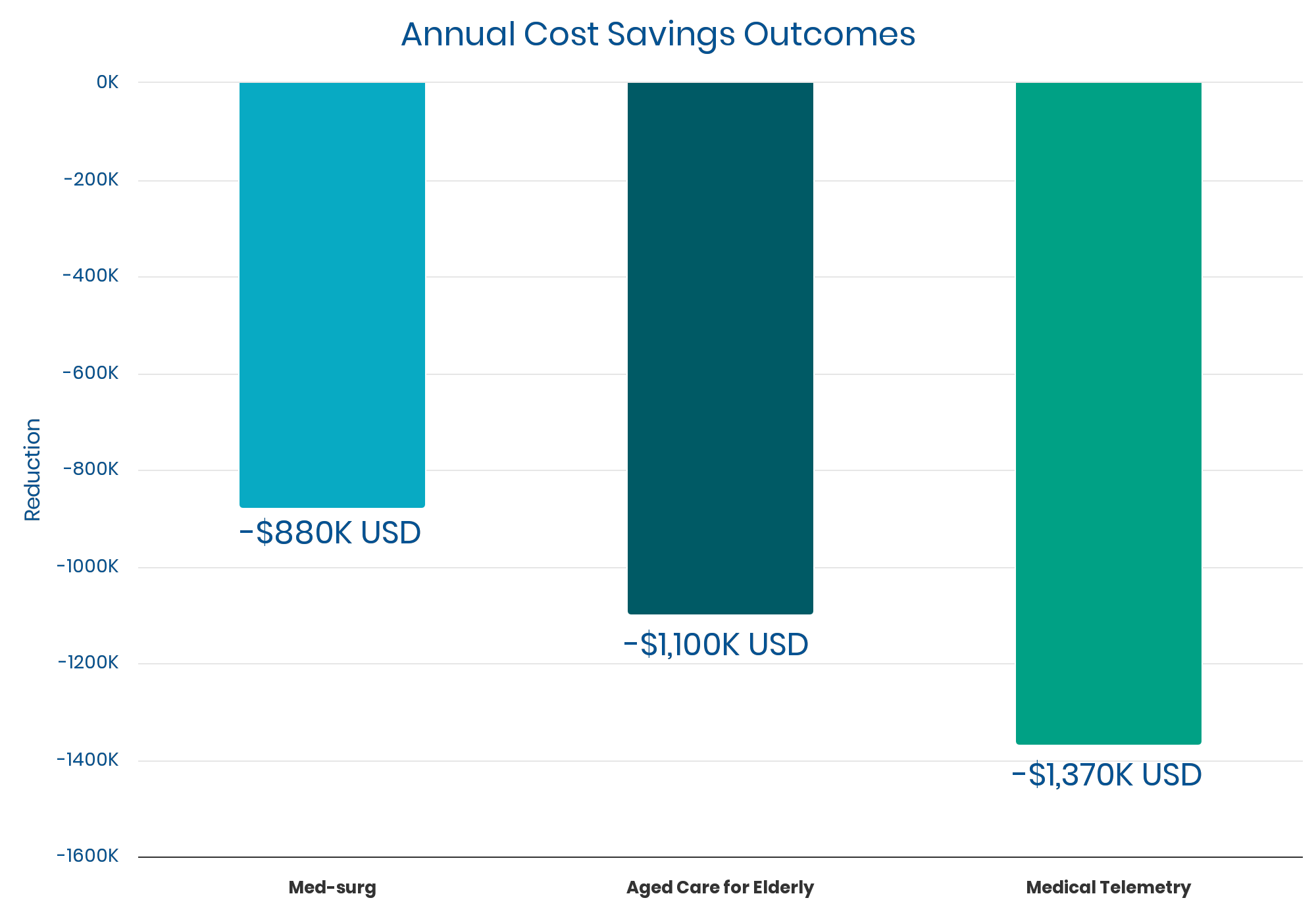
SIBR has some strong outcomes around cost savings, though only 5 sites have published their cost data. Accurate costs of care can be difficult to measure and report, which may explain the paucity of published results.
As noted earlier, there are well-documented Length of Stay decreases averaging 10% to 15%. These are consistent with an observed per-unit cost savings in the rough ballpark of $1,000,000 per year (give or take around 40% depending on unit size). It’s likely that SIBR units with average LOS decreases (10-15%) experience a commensurate level of cost savings (approx. $1,000,000).
One study that used a third-party software tool to measure direct costs per case found a 16% reduction. They did not track additional savings from indirect costs.
Notably, the average cost savings over five years appear to be 10 to 30 times the price of a typical implementation delivered by an external expert. This corresponds to a payback period of 90-120 days for an externally led implementation. A 30x ROI can be compelling – freeing up resources to spend on other priorities.
“Strangely, the chaos in traditional hospitals is still considered normal. Leaders seem genuinely surprised by complications and delays.
So many resources and hours are wasted recovering from what could’ve been prevented in the first place.
This reverses all that and the difference is profound. Every hospital unit should work this way.“